
You are currently browsing the category archive for the ‘Global Crisis Blog’ category.
COVID-19: Lessons from Three Smart Small Asian Nations Part 3. Taiwan
By Shlomo Maital
Taiwan, officially calling itself the Republic of China, is an island nation of some 23.7 million people, with GDP per capita of some $55,000 (using the adjusted exchange rate, known as Purchasing Power Parity), which reflects Taiwan’s undervalued currency.
Taiwan responded very very quickly to the COVID-19 threat, perhaps faster than anywhere:
“Taiwan acted even faster. Like Hong Kong and Singapore, Taiwan was linked by direct flights to Wuhan, the Chinese city where the virus is believed to have originated. Taiwan’s national health command center, which was set up after SARS killed 37 people, began ordering screenings of passengers from Wuhan in late December even before Beijing admitted that the coronavirus was spreading between humans.”
“Having learned our lesson before from SARS, as soon as the outbreak began, we adopted a whole-of-government approach,” said Joseph Wu, Taiwan’s foreign minister. By the end of January, Taiwan had suspended flights from China, despite the World Health Organization’s advising against it. The government also embraced big data, integrating its national health insurance database with its immigration and customs information to trace potential cases, said Jason Wang, the director of the Center for Policy, Outcomes and Prevention at Stanford University. When coronavirus cases were discovered on the Diamond Princess cruise ship after a stop in Taiwan, text messages were sent to every mobile phone on the island, listing each restaurant, tourist site and destination that the ship’s passengers had visited during their shore leave.”
As of Tuesday, Taiwan had recorded 77 cases of the coronavirus, although critics worry that testing is not widespread enough. Students returned to school in late February.
Speed. Agility. Discipline among the population. Preparedness. Anticipation. “Reading the world map correctly”.
This is what we learn from smart, rich, agile, disciplined small Asian nations.
COVID-19: Lessons from Three Smart Small Asian Nations
Part 2. Hong Kong
By Shlomo Maital
Hong Kong is officially known as “the Hong Kong Special Administrative Region of the People’s Republic of China”. It has 7.4 million people and GDP per capita of some $46,000 – higher than that of Israel.
Here, according to the New York Times, is how Hong Kong dealt with the COVID-19 crisis, influenced strongly from its traumatic experience with SARS in 2003:
“ Hong Kong’s heavy death toll from SARS, nearly 300 people, has spurred residents in the semiautonomous Chinese territory to exercise vestigial muscles of disease prevention this time around, even as the local authorities initially dithered on whether to close the border with mainland China. Nearly everyone, it seemed, began squirting hand sanitizer. Malls and offices set up thermal scanners.”
“The most important thing is that Hong Kong people have deep memories of the SARS outbreak,” said Kwok Ka-ki, a lawmaker in Hong Kong who is also a doctor. “Every citizen did their part, including wearing masks and washing their hands and taking necessary precautions, such as avoiding crowded places and gatherings.”
“The Hong Kong government eventually caught up to the public’s caution. Borders were tightened. Civil servants were ordered to work from home, prompting more companies to follow suit. Schools were closed in January, until at least the end of April.”
“On Tuesday, the government of Hong Kong, where only 157 cases have been confirmed, announced a mandatory 14-day quarantine for all travelers from abroad beginning later this week.”
SARS outbreak occurred nearly 17 years ago, in 2003. Despite this, the memory of SARS and the measures adopted at that time are fresh in the minds of Hong Kong citizens. It was the people of Hong Kong who acted, even before the government and administrative officials took action, in the COVID-19 outbreak.
I am certain the same will be true of COVID-19. We will remain this for generations. And hopefully, in the next pandemic, we will act promptly, as Hong Kong did.
COVID-19: Lessons from Three Smart Small Asian Nations Part 1. Singapore
By Shlomo Maital

We can learn a great deal from three small Asian nations or semi-autonomous areas (Hong Kong, Singapore, Taiwan) about how to deal with COVID-19. These lessons are summed up in today’s New York Times, by Hannah Beech:*
Here, Part 1, is how Singapore acted.
I taught MBA students in Singapore, at Nanyang Technological Institute, for many years, and came to know Singapore and its people well.
I can sum up Singapore’s cultural DNA, in place from Day One, in large part thanks to its brilliant founding leader Lee Kwan Yew: We are a small nation, disliked by our huge neighbors. To survive, we must be the very best at everything, and accept no excuses for incompetence.
“Singapore’s strategy of moving rapidly to track down and test suspected cases, provides a model for keeping the epidemic at bay, even if it can’t completely be stamped out completely.
“With detailed detective work, the government’s contact tracers found, among others, a group of avid singers who warbled and expelled respiratory droplets together, spreading the virus…. If you chase the virus, a Ministry of Health official said, you will always be behind the curve.”
Singapore has had a relatively few cases and few deaths, even though the Chinese New Year brought a lot of arrivals from China initially.
The author writes: “Early intervention is the key. So are painstaking tracking, enforced quarantines and meticulous social distancing – all coordinated by a leadership willing to act fast and be transparent.”
Singapore’s key benchmark: To trackers seeking where the COVID-19 was contracted, for those testing positive — you have two hours to bring us concrete answers. Two hours. No excuses.
In Singapore, “details of where patients live, work and play are released quickly online, allowing others to protect themselves.”
Violation of privacy? Embarrassing? Of course. But public health comes first. And a disciplined population accepts this.
[Important correction: My friend Bilahari Kausikan, former senior Foreign Ministry official in Singapore, writes: NYT story was misleading in one detail: it gives the impression that we release the names of the infected. We don’t do that but refer to them by case number. The details are of date, time and places they have visited so that you can be alerted and if you have been there at the material time and date, get yourself checked.”]
Western nations seem to be chasing the virus, after it has arrived, rather than acting pre-emptively well before it unpacks its bags and settles in.
Perhaps next time, we will follow Singapore’s lead?
- “Asian hubs offer model for tackling an epidemic”. New York Times March 19/2020
COVID-19: Why Do More Men Die Than Women?
By Shlomo Maital
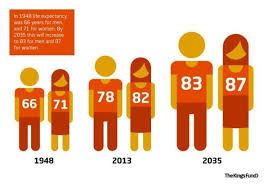
Women live longer than men. It’s true. Here are the facts, from the World Health Organization:
In 2019, more than 141 million children will be born: 73 million boys and 68 million girls.
Based on recent mortality risks the boys will live, on average, 69.8 years and the girls 74.2 years – a difference of 4.4 years.
Life expectancy at age 60 years is also greater for women than men: 21.9 versus 19.0 years.
Women have a longer life expectancy than men at all ages.
Many years ago, when I studied demography at Princeton (at Ansley Coale’s famed Office of Population Research), this fact was true even then – and I read a study of monks and friars, in a monastery, whose life expectancy reflected the same advantage for women – so, it is not environmental factors that cause it.
In fact, we’re not really sure why women live longer. There are many theories.
And now, comes COVID-19. Writing in the daily Haaretz, Asaf Ronal observes that the mortality rate from COVID-19 for men is 2.8%, while the mortality rate for women is 1.7%. That is a massive difference. This is adjusted for age, and other factors.
Why?
There are theories. Behavioral: Men are ‘heroes’ and seek medical care less than women. Physiological: Female hormones protect them. Immunological: Female immune systems work better. Biological: the ‘receptors’ viruses like to invade on human cells reside in part in Chromosome X, women have two copies of it, thus they are more susceptible, so their immune systems are more alert and wary to attack invaders.
These are all theories. None have really been fully tested.
And finally, my own observation: As we observe spatial separation here in Israel, and as I watch both men and women experts explain things and advise us on TV – again, as always, I am struck by how much better women are at delivering information, credibly, authentically, than men, given the same level of expertise and training.
If only the men would leave it to the women – and just shut up. US President, are you listening? And Israeli PM? Men — take care of yourselves. Let the women run things. They do it better.
COVID-19: AI to the rescue?
By Shlomo Maital

Today’s daily Haaretz * carries a brief report of how three brilliant Israeli scientists have tackled a pressing problem – the need to know where the COVID-19 hotspots are, in order to focus spatial separation without shutting down the economy of the entire country.
The three are Prof. Eran Segal, an expert in computational and systems biology, Weizmann Institute, Rehovot; Prof. Benny Geiger, also from Weizmann; and Prof. Yuval Dor, Hebrew University.
Segal notes that experience from studying previous epidemics, as well as knowledge about how COVID-19 spreads, show that the virus spreads through clusters of infection and that early identification of such clusters can help stop the virus from spreading, ot at least slow it considerably.
We have seen such clusters, or hot spots, in New Rochelle, NY, in Washington State (Seattle), and initially, in Wuhan, China.
Segal notes that one possibility is to use massive testing, as they did in South Korea. More than 10,000 persons are tested daily there for COVID-19.
Israel can’t do such extensive testing, at this stage, he notes. Hence, the solution the team found was to ask members of the public to fill out online daily questionnaires, which take less than two minutes to complete, that include details about various symptoms and place of residence, including street and zip code.
This information will be analyze, Segal notes, using machine learning algoithms that give researchers and the Health Ministry a variety of information. If enough data are collected, the tool will help give up-to-date assessment of the spread of the illness.
This ‘early warning’ system can help spot these clusters, long before other methods do. The AI algorithms could also determine the effectiveness of public health measures, such as self quarantine, to limit COVID-19’s spread.
The information, noted Segal, is collected using Google DOCS. No privacy is violated.
Segal says we need as many people as possible to fill out the questionnaire, in the initial pilot stage.
I wonder whether Israel can offer this approach to the US, where testing remains quite limited.
* Haaretz. “Israeli Researchers Hope AI Can Tame COVID-19, and They Want Our Help.” Asaf Ronel. March 17 2020.
Why Don’t Kids Get COVID-19?
By Shlomo Maital

Why does the COVID-19 virus afflict us seniors, but small children seem immune?
Today’s Haaretz daily has an interesting article by science writer Asaf Ronal, addressing this question.
First, the data, from Worldometers. The probability of death from COVID-19, by age group: 21.9% of those 80+, 8% for those 70-79, 3.6% for those 60-69, 1.3% for those 50-59, 0.4% for those 40-49, 0.2% for those 30-39, 0.2% for those 20-29, 0.2% for those 10-19….. and, amazingly, zero %, for those 0-9. (No known fatalities, among the world’s 180,000 cases, for young children)!.
Why?
Here are the five main hypotheses.
- Young kids have more flexible, adaptable immune systems, better able to adapt to new diseases, because this is what kids’ immune systems are learning to do from the start.
- Young kids have a much smaller number of ‘damaged’ immune cells…such cells are more susceptible to the invasion of COVID-19 clever viruses, whose spikes poke into cells and invade them.
- Young kids’ cells have far fewer ‘receptors’, that viruses use to penetrate them and reproduce inside them.
- Young kids’ lungs have surface membranes that are far less likely or susceptible to ‘housing’ the virus and enabling them to reproduce there.
- Young kids still do not have the sex hormones, that may induce proteins in human cells that help the viruses reproduce, when they get inside those cells.
We don’t know which, if any, of these theories is the right one. One day, maybe soon, we will find out – and perhaps that will help us old seniors as well.
Social Isolation? No! Spatial Separation: Yes!
By Shlomo Maital

My wife is a school psychologist, with long experience, including times of emergency, when Israel was under attack.
She has an important observation regarding the widespread calls for “social isolation”, to maintain distance among us and slow the spread of the coronavirus.
I want to share her observation.
Words matter. The last thing we need in times of crisis is “social isolation”. This is especially true of my country Israel. As Judy Meltz notes in today’s Haaretz daily, “In a country where personal space is virtually nonexistent, many Israelis are struggling”. We are a touchy-feely nation, in good times we fight like hell, and in hard times we pull together and help one another.
So how in the world are we to manage ‘social isolation’?
Answer: Words matter! This is NOT social isolation. We are still in close touch by social media. Our own family Whatsapp is feverishly active.
What we are called to do is simply spatial separation. Separate one another in space. That does not mean isolating one another socially.
Look, words do matter. I hope our leaders will embrace this term, spatial separation, which is precisely what it is, and abandon ‘social isolation’. Let’s support one another constantly, despite being physically separated.
Thank you, Sharona.
Love in the Time of COVID-19: Learning from Boston
By Shlomo Maital

Love in the Time of Cholera (in Spanish: El amor en los tiempos del cólera) is a novel by the Colombian Nobel prize winning author Gabriel García Márquez. First published in 1985, an English-language movie adaptation was released in 2007.
In the novel, a young national hero, Dr. Juvenal Urbino, meets Fermina and begins to court her. Despite her initial dislike of Urbino, Fermina gives in to her father’s persuasion and they marry. Urbino is a physician devoted to science, modernity, and “order and progress”. He is committed to the eradication of cholera and to the promotion of public works. He is a rational man whose life is organized precisely and who greatly values his importance and reputation in society. He is a herald of progress and modernization and the love of others.
It’s a good time, as many of us hang out at home, to reread this novel. Because, there is a great deal of love in the time of COVID-19.
Utah Jazz star Rudy Gobert, who has COVID-19, joked on-line about it, thrust microphones at journalists, purposely touched surfaces – the kind of bravado that athletes often show in the time of danger and fear. The public reaction was fiercely negative. Govert has apologized and donated $500,000 to COVID-19 victims.
Christiano Ronaldo, perhaps the world’s greatest football player, is at home, in Portugal (Madeira), in his incredible pad – but announced that he is converting the hotel chain he owns into hospitals, at his personal expense.
But these two are celebs. What about ordinary people?
I am very fond of Boston, MA., having taught 20 summers there, at MIT. “Boston strong” was the city’s reaction to the terrible bombing at the Boston Marathon.
Now, Boston radio station WBZ reports on these acts of kindness, by ordinary people:
* Norfolk/Worcester County restaurants feed kids for free It started with Goodstuff Smokehouse in Blackstone, MA announcing “any student that comes in during weekday lunchtime (parents or not) will be given a free kids meal togo. No questions asked. We will continue to do this until area schools are back to normal.”That generous idea has since caught on among several other local eateries, including PJ’s Smoke ‘N’ Grill in Medway, and 140 Pub N Club in Bellingham.
Many kids in the US are fed in schools…some, breakfast lunch and dinner. Closing the schools can bring hunger to these kids. Time for others to step up, including restaurants, that are empty anyway.
* The Greater Somerville Homeless Coalition is raising money to help some of the people who are at the highest risk for catching coronavirus; Boston’s homeless population. Since the outbreak of coronavirus forced them to cancel their Gala, the Somerville Coalition has taken their fundraiser online. As of Saturday afternoon the Coalition is more than $13,000 towards its $70,000 goal. To help support Boston’s homeless population during the COVID-19 outbreak, click here.
* A group called Violence In Boston Inc. is providing free meals for BPS kids, and is accepting donations to help low income families around Boston impacted by the coronavirus pandemic. Starting Sunday March 15 until Friday March 20, volunteers will be collecting supplies like soap, toilet paper, and hand sanitizer to donate to Boston’s families in need. They will be serving lunch and dinner for any BPS child in need of a meal.
* Thanks to the Charles River Mutual Aid Program, activists from various universities are mobilizing to provide mutual aid to students and other Boston-area residents who are in need of resources amid the COVID-19 outbreak. For students who have been kicked off their campuses, the organization will try to provide housing and storage space, although it is limited. They will be pooling funds in a Mutual Aid Fund to purchase food, medical supplies, and other necessities, and organizing to provide these resources to the community. When universities decreed hasty closing, and emptied the dorms, they have not given thought to students who have nowhere else to live.
* The Boston Music Maker Relief Fund has been set up by The Record Co. to help Boston-based musicians whose work has been impacted by the coronavirus outbreak. The organization will pay out $200 relief grants on a first come first serve basis.
* A Harvard Med Group Is Caring For The Senior Population. A group from Harvard Medical School says it is “making itself a hub for local efforts to care for the aged, isolated & needy during coronavirus.”
* The so-called Neighborhood Aid Network is helping people in need from Cambridge to Jamaica Plain by helping pick up groceries, giving rides to doctors appointments, and simply letting people know they are not alone.
There is a terrible paradox in how we must react to COVID-19: Social and individual resilience is driven by our network of love and support, among family friends and even strangers. Yet we are asked to maintain ‘social separation’ – the exact opposite. We will find ways to navigate this dilemma and come through it. Meanwhile, love in the time of COVID-19 will triumph over fear, panic and shelf-emptying hoarding.
Can each of us think of some small way to spread love (not virus) in the time of COVID-19?
COVID-19: Mitigate, Not Decimate
By Shlomo Maital

Professor Zvi Bentwich is an Israeli doctor, who teaches and researches at Ben Gurion University, in Beersheva. Before quoting his views on COVID-19, let me establish his credentials first.
Bentwich serves as the head of the Center for Emerging Tropical Diseases and AIDS at the Ben-Gurion University (BGU). He founded the first AIDS center in Israel in the mid 80’s. His groundbreaking research uncovered the link between Neglected Tropical Diseases (NTDs) , particularly intestinal worms, and immune system deficiencies, pioneering the concept that NTDs play a major role in the pathogenesis of HIV/AIDS. He is a leading advocate for public health and human rights.
So, this is a public health expert who is worth listening to, right? Here is his take, printed in today’s Haaretz daily newspaper:
The heading on his Op-Ed piece: “Tight border isn’t the answer to virus”. Today the Israeli government announced that EVERYone returning from abroad must undergo self-imposed quarantine for two weeks. Everyone? Yes, so that Prime Minister Netanyahu will not appear to be singling out the US, thus angering his friend and colleague Donald J. Trump. (Such quarantines were already in effect for most travellers incoming from Europe).
The main point: “Is there an alternative approach to fighting the disease right now? [alternative, to closing down the borders and shutting down the economy for weeks and weeks?]. …Yes, it’s clale mitigation. It involves using less drastic methods that are likely to yield similar results regarding the damage caused by the virus but that significantly reduce the negative social and econoic consequences of containment.”
Mitigation. Not decimation of our economy.
And this is coming from a distinguished physician, expert on virus containment.
Bentwich concludes: “The coronavirus too will pass and until it does the damage should be minimized as far as possible. We must accept the possibility that it won’t be the last viral epidemic and that it’s important to find the optimal way to cope with such epidemics, at a reasonable cost”.
COVID-19: Calibrate Your Risk Perception
By Shlomo Maital
How risky is COVID-19 to me, personally? How do I process the news, numbers, fake news, and hysteria, to evaluate the seriousness of the threat to me, personally?
Behavioral economics knows a lot about risk perception. Many years ago, Kahneman and Tversky showed, with simple this-or-that choice experiments, that we humans overwhelmingly overestimate small probabilities.
This seems to be the case with COVID-19. Writing in the New York Times, medical doctor and psychiatrist Richard Friedman observes: *
Throughout the country, people are stockpiling food in anticipation of a shortage or a quarantine. Supplies of Purell hand sanitizer flew off the shelves in local pharmacies and are now hard to find or even unavailable online. I understand the impulse to secure one’s safety in the face of a threat. But the fact is that if I increase the supply of medication for my patients, I could well deprive other patients of needed medication, so I reluctantly declined those requests. As a psychiatrist, I frequently tell my patients that their anxieties and fears are out of proportion to reality, something that is often true and comforting for them to realize. But when the object of fear is a looming pandemic, all bets are off.
Friedman continues:
In this case, there is reason for alarm. The coronavirus is an uncertain and unpredictable danger. This really grabs our attention, because we have been hard-wired by evolution to respond aggressively to new threats. After all, it’s safer to overact to the unknown than to do too little. Unfortunately, that means we tend to overestimate the risk of novel dangers. I can cite you statistics until I am blue in the face demonstrating that your risk of dying from the coronavirus is minuscule compared with your risk of dying from everyday threats, but I doubt you’ll be reassured. For example, 169,000 Americans died by accident and 648,000 died of heart disease in 2017, according to the Centers for Disease Control and Prevention. As of Sunday morning 19 Americans had died from the coronavirus.
OK – so what SHOULD we be doing, then, in the face of panic that the objective risk does not justify?
Find ways to help and reassure others, notes the wise Dr. Friedman.
Researchers found that when subjects made selfish decisions, the brain’s reward center was activated, whereas when they made generous decisions, a region of the brain implicated in empathy lit up. This suggests that people are more likely to be altruistic if they are primed to think of others and to imagine how their behavior might benefit them.
The good news is that even in the face of fear, we do have the capacity to act in ways that would help limit contagion during an epidemic. Specifically, we can behave altruistically, which benefits everyone. For example, research shows that when people are told that it is possible — but not certain — that going to work while sick would infect a co-worker, people are less willing to stay home than when they are reminded of the certainty that going to work sick would expose vulnerable co-workers to a serious chance of illness. Stressing the certainty of risk, in other words, more effectively motivates altruism than stressing the possibility of harm The lesson for the real world is that health officials should be explicit in telling the public that selfish responses to an epidemic, such as going to work while sick or failing to wash your hands, threaten the health of the community.
And what should our great leaders do?
Specifically, public figures need to convey loudly and clearly that we should not go to work or travel when we’re sick and that we should not hoard food and medical supplies beyond our current need — not just give us health statistics or advise about how to wash our hands.
Let us all try to recalibrate our risk perceptions. COVID-19 will spread, it will afflict a lot of people, it IS NOT possible to put it back in Pandora’s box. But there are a lot of other scary things going on in this world that threaten each of us. Because we have known them for a long time (ordinary flu, traffic deaths, etc.), we are habituated. COVID-19 is new, scary and rather unknown. We will in time come to know it. We will overcome it. And in the meantime, help and reassure your family and your friends. Take it from Dr. Friedman.
* “The Best Response to the Coronavirus? Altruism, Not Panic. The impulse to secure your safety is understandable but counterproductive.” by Dr. Richard A. Friedman, NYT March 8/2020

