
You are currently browsing the tag archive for the ‘COVID-19’ tag.
Two Turks and a Greek Collaborate – And Save the World
By Shlomo Maital

Dr. Uğur Şahin and Dr. Özlem Türeci
Every major nation in the world is feverishly working to develop a vaccine against COVID-19. Billions of dollars have been spent, thousands enlisted, politics pollutes science — and in the end, the world will be saved by two brilliant people whose families emigrated from Turkey to Germany, together with a Greek CEO. Here is the story, based on David Gelles’ New York Times article.*
*David Gelles. They’re first in the face for a vaccine. NYT, Friday Nov. 13, 2020, p. 8
On Monday Nov. 9, Pfizer announced that a COVID-19 vaccine developed by Dr. Ugur Sahin and Dr. Ozlem Tureci had been shown to be over 90% effective. Predictably, Trump claimed falsely that the announcement had been purposely delayed to harm his re-election. The announcement was made by Albert Bourla, Pfizer CEO, who is Greek. What lovely irony that two Turks and a Greek combine to save the world!
Who are Ugur Sahin and Ozlem Tureci?
Sahin, 55, was born in Iskendurun, Turkey. His family moved to Cologne, Germany, when he was 4; his parents worked in a Ford car factory there. He graduated from the Univ. of Cologne as a medical doctor and later, Ph.D., after researching immunotherapy for caner. He met Dr. Tureci, 53, early in his career; she hoped to become a nun, but ended up studying medicine; she was the daughter of a Turkish physician who emigrated to Germany from Istanbul.
In 2001 Sahin and Tureci founded Ganymet Pharmaceuticals to develop monoclonal antibodies to treat cancer. [A monoclonal antibody is made by cloning a unique white blood cell, that bind to an antigen, e.g., a virus, cancer cell or bacteria and keep it from making us ill]. They sold Ganymet for $1.4 billion in 2016.
As billionaires, did they go off to bask on a beach in the Bahamas?
Far from it. They founded BioNTech, even before selling Ganymed, to use messenger RNA (mRNA) (see below) to treat cancer.
What insight did Dr. Sahin have two years ago?
At a conference in Berlin, Sahin told a roomful of infectious disease experts, that his company BioNTech “might be able to use messenger RNA to create a vaccine in the event of a global pandemic.” BioNTech began work on the vaccine in January, after Sahin read an article in a medical journal and saw how the novel coronavirus was about to spread worldwide. Scientists at BioNTech cancelled vacations and went to work on what they called Project Lightspeed (Trump copied Warpspeed from them).
What is an mRNA vaccine?
This is brand-new vaccine technology. “To produce an mRNA vaccine, scientists produce a synthetic version of the mRNA (RNA, ribonucleic acid, is a molecule vital in genetic coding and decoding) that a virus uses to build its infectious proteins. This mRNA is delivered into the human body, whose cells read it as instructions to build that viral protein, and therefore create some of the virus’s molecules themselves. These proteins are solitary, so they do not assemble to form a virus. The immune system then detects these viral proteins and starts to produce a defensive response to them.” This is a relatively new technology for creating vaccines. No such vaccine existed before.
What role does Pfizer play?
BioNTech developed the vaccine. But the process of clinical testing, passing regulation, and producing billions of doses, needed a Big Pharma company. BioNTech has been collaborating with Pfizer since 2018. Pfizer CEO Albert Bourla was born in Thessaloniki, Greece and has been with Pfizer since 1992. In March BioNTech and Pfizer signed a collaborative agreement.
Is BioNTech a major company?
It is now! Its market value has understandably soared, to over $21 billion, and it is based in Mainz, Germany, employing 1,323. This makes Sahin and Tureci among Germany’s wealthiest persons. However, they live in a modest apartment, with their teenage daughter, and bicycle to work. They do not own a car.
Will the BioNTech mRNA vaccine save the world?
Maybe. But a major problem will be transporting it. It requires cooling to minus 70 degrees C. Even major hospitals do not have storage facilities for a vaccine at that ultra-low temperature. The vaccine will have to be shipped in dry ice (solid frozen CO2), which is minus 78.5 degrees C.
COVID-19 Leaders: Listen to the Women
By Shlomo Maital

I’ve written this before – but now, today, with the coronavirus raging in the US and EU – it bears repeating. Women have done far far better than men, as national leaders in the fight against the pandemic. Question is – why? *
* see Arwa Mahdawi, “the secret weapon in the fight against coronavirus: women”. The Guardian, April 11 2020.
* Tsai In-Wen, a former lawyer, Taiwan’s first female President elected in 2016, has effectively limited the pandemic in her country, from the start.
* Jacinda Arden has virtually eliminated the coronavirus in New Zealand and won resounding re-election, with a parliamentary majority.
* Angela Merkel, lame-duck German Chancellor, has been a voice of calm and reason, in the face of neo-Nazi demonstrations in her country. She is herself a scientist, and not only listens to the science but truly deeply understands it.
* Denmark, led by PM Mette Frederiksen, and Finland, led by PM Sanna Marin, have both done well in limiting the pandemic in their countries.
* As of 27 September 2020, Norway has performed 1,034,670 tests and reported 13,741 confirmed cases and 274 deaths. A senior Norwegian Institute of Public Health consultant said one of the major reasons why the mortality rate was significantly lower than in other European countries (such as Italy, Spain, the UK) was the high number of tests performed in Norway. Erna Solberg has been Norwegian PM for over 6 years.
* Iceland joins Taiwan, mong a group of countries which adopted a cooperative strategy early on in the pandemic, bringing together multiple organizations to tackle the challenges in containing COVID-19. Katrín Jakobsdóttir is erving as the 28th and current Prime Minister of Iceland since 2017.
Seven brilliant women, who have led their countries to safe shores. Concidence? When the three biggest failures in controlling the pandemic were led by men: Trump (US), Bolsinaro (Brazil) and Johnson (UK)?
I could list some speculative theories about why women have been far more successful than men in controlling the pandemic crisis.
But I leave it to the reader. Because – you, dear reader, know why.
Mental Health Impact of COVID-19: A Survey of 59 Countries
By Shlomo Maital

We are approaching almost a year of the coronavirus pandemic – and in virtually every country (except perhaps New Zealand, where fans are filling stadiums to watch the All-Blacks), it is beginning to wear people down. Here are the results of large-scale study of the mental health impact, based on a sample of 6,882 individuals in 59 countries. *
- Elisabet Alzueta et al., “How the COVID-19 Pandemic has changed our lives: A study of psychological correlates across 59 countries”. J. of Clinical Psychology 2020: 1-15.
Of the nearly 7,000 participants, 25.4 % reported moderate-to-severe depression, while 19.5% reported anxiety symptoms.
What caused the depression? A variety of factors: Among them,
* the country’s income level (higher income correlated with higher depression), * exposure to COVID-19 (e.g. unconfirmed symptoms), * government lockdowns, * life changes (e.g. working from home); and * conflicts with other adults at home. However, all these factors ‘explained’ (in a statistical sense) only about one-fifth of the variance in depression.
A major battle is underway between the “the cure (of the pandemic) is worse than the disease, let’s open at once” camp, and the “you cannot heal the economy until you stamp out the damned virus” camp. I think the latter are more right – better to severely lock down, like taking a very bitter medicine to cure an illness, to shorten the prolonged impact on mental health by failing to do so.
It is surreal that American voters are basically being asked to choose between these two camps, Trump vs. Biden — when the issue is really rooted in complex epidemiology and shrouded in massive uncertainty. It is clear, however, that the science and the scientists overwhelmingly favor the “end the virus first, clamp down hard” policy.
Post-Pandemic Youth: Tired But Hopeful
By Shlomo Maital

A great many hard words have been said and written about GenY and GenZ, the young generations – who are tired of lockdown and perhaps spread virus to vulnerable elderly.
Here is a different take, based on a survey of 1,300 full-time college students in the US, UK and Canada, published in Harvard Business Review.*
- A. Whillans, L.M.Giurga, L. Macchia and A. Yemisoigil, “Why a Covid-19 World Feels Both Tiring and Hopeful for College Students”. Harvard Business Review, August 3, 2020.
The main finding, is this:
“Many students also demonstrated a heightened concern for helping others and hoped to find work that fulfilled a greater purpose. Specifically, students reported a heightened interest in pursuing careers that were useful to society and that helped other people. The single highest job priority for the college students we studied was “to have a job that allowed them to help other people.” In light of the economic recession, perhaps unsurprisingly, students’ desire to have a purposeful career was followed closely by “having a job that resulted in high income” and “job security.” Perhaps most interesting was the fact that prosocial and economic-based career motivations were stronger in this student sample than opportunities for advancement, job flexibility, and free time: three motivations which typically dominate career interests among this age group.
The pandemic has taken a terrible of lives and sickness, among millions. But in a way, it has also been a global alarm clock, a wake-up call. And perhaps, according to this Harvard study, it has resonated especially with younger people. This is crucial, because it is they who will “Build Back Better”. Older generations sometimes teach the younger ones – but perhaps, today, it is the elderly who can learn from the young.
The authors conclude:
We are all exhausted and stressed. Perhaps more than any other group, students are especially concerned with what the future holds. Yet, we can all learn something from our data and this moment. Using this present as a chance to reflect about life’s meaning, and our own desired legacy, can increase our resilience in facing our unknown challenges. In becoming more resilient and reflective, we will not only reduce our own personal stress, but also become more focused on helping our families, our communities, and our country.
COVID-19 Immunity: Is It Short-Lived?
By Shlomo Maital

One crucial fact we need to know and understand about COVID-19 — for those who have had it, and survived – are they immune? For how long?
Now comes a study from England, that is not good news at all. According to Nicola Davis, writing in The Guardian:
“The proportion of people in England with coronavirus antibodies dropped by more than a quarter in the space of three months, researchers have revealed, fueling concerns over reinfection. The findings come from the React-2 study, which is based on home finger-prick antibody test results from random participants across all 314 local authorities. The first results, based on data from 100,000 people, were released in August, revealing that about 6% of the population of England had the antibodies – protective proteins produced in response to an infection – although the team say that could be a slight underestimate. The new work – not yet peer-reviewed – extends this with more testing in two fresh cohorts, each yielding results from more than 100,000 adults. The results reveal that just 4.4% of those tested in the most recent round, between 15 and 28 September, had detectable coronavirus antibodies.
“As a whole, these data suggest the possibility that decreasing population immunity will lead to an increased risk of reinfection as detectable antibodies decline in the population,” said Graham Cooke, co-author of the report and professor of infectious diseases at Imperial College London.“
Apparently, too, the elderly lose immunity faster than do the young.
This does NOT mean that a COVID-19 vaccine will be ineffective. “… the new results do not necessarily mean that immunity arising from vaccination would be short-lived. A good vaccine may well be better than natural immunity.
So what do the British results imply, for ordinary citizens? I think they mean — hunker down, everyone, this novel coronavirus is going to be with us for a long time, and we are going to have to learn to co-exist with it. Masks, some social distancing, etc. We are resilient. We CAN live with it.
The crucial point is, to live with it, not die with it. Those who scorn what science and public health tell us to do, are potentially guilty of “negligent homicide”, a well-defined crime in criminal law.
Why Rwanda Is Far Smarter Than the US –
Dealing with COVID-19
By Shlomo Maital

Consider Rwanda. This small African country in south-central Africa, landlocked, has about 12 million people, with GDP per capita of about $2,600. This is only 4% of America’s per capita GDP. So Americans are 25 times wealthier than Rwandans…. But – is the US leader as smart as Rwanda’s, Paul Kagame? 4% as smart?
Rwanda has struggled to move beyond the terrible massacre/genocide that occurred between April and July 1994, which killed between half a million and a million Tutsi – 70% of the total Tutsi population in Rwanda.
Here is how Jason Beaubien, National Public Radio, described Rwanda’s success in controlling COVID-19. First the numbers:
| Cases
4,789 |
Recovered
3,080 |
Deaths
29 |
Now Beaubien:
“A robot introduces itself to patients in Kigali, Rwanda. The robots, used in Rwanda’s treatment centers, can screen people for COVID-19 and deliver food and medication, among other tasks. The robots were donated by the United Nations Development Program and the Rwanda Ministry of ICT and Innovation.
“In some places in the world right now, getting tested for COVID-19 remains difficult or nearly impossible. In Rwanda, you might just get tested randomly as you’re going down the street.
“So whenever someone is driving a vehicle, bicycle, motorcycle or even walking, everyone is asked if you wish to get tested,” says Sabin Nsanzimana, director general of the Rwanda Biomedical Center, which is the arm of the ministry of health that’s in charge of tackling COVID-19. Health officials in personal protective equipment administer the test. Nsanzimana says the testing is voluntary, although some others say refusal is frowned upon.
“The sample collection — from a swab up the nose — and filling out the contact information paperwork takes about five minutes.
“All these samples are sent that day to the lab,” Nsanzimana says. “We have a big lab here in Kigali. We have also six other labs in the other provinces.”
“Despite being classified by the World Bank as a low-income country, and despite its limited resources, Rwanda has vowed to identify every coronavirus case. Anyone who tests positive is immediately quarantined at a dedicated COVID-19 clinic. Any contacts of that case who are deemed at high risk are also quarantined, either at a clinic or at home, until they can be tested.
Kagame is controversial; he is accused of being dictatorial and anti-democratic. That may be. But he and his country have done much much better than the wealthy United States, in protecting its citizens.
Remember what President Trump called some African countries? In 2018? S???hole countries? Hmmm.
SARS-COV-2 Has One Big Trick – Have We Just Discovered It?
By Shlomo Maital

According to the India Times’ Economic Times: SARS-COV-2 virus has one big trick – and it may be that scientists have just figured out what it is.
“It looks like this virus has one big trick,” said Shane Crotty, a professor in the Center for Infectious Disease and Vaccine Research at the La Jolla Institute for Immunology in California. “That big trick is to avoid the initial innate immune response for a significant period of time and, in particular, avoid an early type-1 interferon response.”
According to the India Times: The work highlights the potential for interferon-based therapies to enlarge a slowly accumulating range of Covid-19 treatments. These include Gilead Sciences’ remdesivir and convalescent plasma, a component of the blood of recovered patients that may contain beneficial immune factors. These treatments provide limited benefit and are typically used in very sick, hospitalized patients. The possibility that interferon may help some people is enticing because it appears most efficacious in the early stages of infection when life-threatening respiratory failure could still be averted. Dozens of studies of interferon treatment are now recruiting Covid-19 patients.
How did the scientists figure this out? Here is the story:
When two brothers fell critically ill with Covid-19 around the same time in March, their doctors were baffled. Both were young — 29 and 31 years old — and healthy. Yet within days they couldn’t breathe on their own and, tragically, one of them died. Two weeks later, when a second pair of Covid-stricken brothers, both in their 20s, also appeared in the Netherlands, geneticists were called in to investigate. What they uncovered was a path leading from severe cases, genetic variations and gender differences to a loss of immune function that may ultimately yield a new approach to treating thousands of coronavirus patients. The common thread in the research is the lack of a substance called interferon that helps orchestrate the body’s defence against viral pathogens and can be infused to treat conditions such as infectious hepatitis. Now, increasing evidence suggests that some Covid-19 patients get very ill because of an impaired interferon response. Landmark studies published on Thursday in the journal Science showed that insufficient interferon may lurk at a dangerous turning point in SARS-CoV-2 infections.
See also:
“Impaired type I interferon activity and inflammatory responses in severe COVID-19 patients” Science 07 Aug 2020: Vol. 369, Issue 6504, pp. 718-724
COVID-19 Vaccines: What We Know
By Shlomo Maital

In my country Israel, there are more new daily cases per million population than anywhere in the world. Europe too is undergoing a second wave; and many states in the United States are also seeing increasing morbidity. So – everywhere, we await a vaccine.
Over a hundred different efforts are underway to create, produce and administer COVID-19 vaccines. Here is what we know so far, based on a very clear, lucid website sponsored by the Children’s Hospital of Philadelphia. This vaccine effort is an amazing global effort, led by the top scientific minds, trying a wide variety of creative approaches, some tried and true, some radical and innovative. One or more of them will save humanity!
What types of vaccine are being tested?
Several.
* Inactivated vaccine — The whole virus is killed with a chemical and used to make the vaccine. This is the same approach that is used to make the inactivated polio (shot), hepatitis A and rabies vaccines;
*Subunit vaccine — A piece of the virus that is important for immunity, like the spike protein of COVID-19, is used to make the vaccine. This is the same approach that is used to make the hepatitis and human papillomavirus vaccines.
* Weakened, live viral vaccine — The virus is grown in the lab in cells different from those it infects in people. As the virus gets better at growing in the lab, it becomes less capable of reproducing in people. The weakened virus is then used to make the vaccine. When the weakened virus is given to people, it can reproduce enough to generate an immune response, but not enough to make the person sick. This is the same approach that is used to make the measles, mumps, rubella, chickenpox and one of the rotavirus vaccines.
* Replicating viral vector vaccine — In this case, scientists take a virus that doesn’t cause disease in people (called a vector virus) and add a gene that codes for, in this case, the coronavirus spike protein. Genes are blueprints that tell cells how to make proteins. The spike protein of COVID-19 is important because it attaches the virus to cells. When the vaccine is given, the vector virus reproduces in cells and the immune system makes antibodies against its proteins, which now includes the COVID-19 spike protein. As a result, the antibodies directed against the spike protein will prevent COVID-19 from binding to cells, and, therefore, prevent infection. This is the same approach that was used to make the Ebola virus vaccine.
* Non-replicating viral vector vaccine — Similar to replicating viral vector vaccines, a gene is inserted into a vector virus, but the vector virus does not reproduce in the vaccine recipient. Although the virus can’t make all of the proteins it needs to reproduce itself, it can make some proteins, including the COVID-19 spike protein. No currently licensed vaccines use this approach.
* DNA vaccine — The gene that codes for the COVID-19 spike protein is inserted into a small, circular piece of DNA, called a plasmid. The plasmids are then injected as the vaccine. No currently licensed vaccines use this approach.
* mRNA vaccine — In this approach, the vaccine contains messenger RNA, called mRNA. mRNA is processed in cells to make proteins. Once the proteins are produced, the immune system will make a response against them to create immunity. In this case, the protein produced is the COVID-19 spike protein. No currently licensed vaccines use this approach.
Which type of COVID-19 vaccine is most likely to work?
It is likely that more than one of these approaches will work, but until large clinical trials are completed, we won’t know for sure. Likewise, the different approaches may have different strengths and weaknesses. For example, mRNA or DNA vaccines are much faster to produce, but neither has been used to successfully make a vaccine that has been used in people. On the other hand, killed viral vaccines and live, weakened viral vaccines have been used in people safely and effectively for many years, but they take longer to produce.
In addition to differences in how long it takes to make different types of vaccines, each type may also cause the immune system to respond differently. Understanding the immune responses that are generated will be important for determining whether additional (booster) doses will be needed, how long vaccine recipients will be protected, and if one type offers benefits over another.
Is one of the COVID-19 vaccines expected be more effective for the elderly population?
It is likely that COVID-19 vaccines could have different levels of effectiveness in various subgroups of people. Because the elderly generally do not respond as well to vaccines, one or more COVID-19 vaccines may not work well for them, which is concerning given their higher risk of severe disease. The large phase III studies may not include people over a certain age. But, the manufacturers have been encouraged to include older people, so that we have this type of information earlier in the process than may usually occur. We will have to wait and see what the data show to know which vaccine(s) work best in the older population.
How many doses of a COVID-19 vaccine will be needed? Will a booster dose be needed?
The number of doses of a COVID-19 vaccine that will be needed has not yet been determined. The coronavirus vaccines being studied are evaluating one or two doses. When giving two doses, they are usually given one or two months apart. We will need to wait for the results of the clinical trials to have more information about how many doses will be needed.
How long will vaccine immunity last?
Since we do not yet know how long immunity after infection lasts, immunity following vaccination will also have to be determined. Likewise, immunity following vaccination will depend in part on which types of vaccines are licensed, what part of the immune system responds to the vaccine, and the level of immunity that is generated by the vaccine.
If more than one vaccine becomes available, could taking two different vaccines boost the effectiveness?
While it is likely that more than one COVID-19 vaccine will become available, we probably won’t have a good answer to this question until vaccines are actually licensed and we know more about them. Three scenarios can occur if a person is vaccinated with two versions of vaccines against the same disease, particularly close in time:
— They get a stronger immune response. An example of this was when children got inactivated polio vaccine and later got oral polio vaccine.
—- The second vaccine causes immunity that would be similar to receiving a second dose of the original vaccine. Using a different brand of hepatitis B vaccine for one or more doses would be an example of this.
— The immune response generated by the first vaccine interferes with components of the response to the second vaccine, in some cases causing lower immunity. For example, when people got a pneumococcal polysaccharide vaccine (PPSV) followed by a pneumococcal polysaccharide vaccine with a harmless helper protein attached to it, called pneumococcal conjugate vaccine (PCV), they had lower antibody responses to one part of the PCV vaccine than people who got the two vaccines in the opposite order (PCV followed by PPSV).
For these reasons, studies will need to be done to determine the effects of getting a second type of COVID-19 vaccine shortly after receiving a different one. If, however, we find that COVID-19 vaccines are like influenza vaccines and we need to get vaccinated annually, concerns about switching types from one year to the next are less likely to be an issue.
Will a coronavirus vaccine need to be given annually?
When a vaccine is licensed, we will only have information about length of immunity for as long as we are from the trials. For example, if the first people in the study were vaccinated in July 2020 and the vaccine is licensed in December 2020, we will only have information about the immune response up to 5 months after vaccination. The vaccine manufacturer will likely continue to monitor vaccine recipients for several months or more, so that over time, we will continue to get a better picture of the durability of immunity. With this information, we will be better able to understand whether vaccines against COVID-19 will require annual dosing like influenza.
Is a coronavirus vaccine necessary?
SARS-CoV-2 infections can be a minor hindrance or lead to severe disease or even death. While hygiene measures such as social distancing, handwashing, and wearing masks offer some help, the best way to stop this virus is to generate SARS-CoV-2-specific immunity. This specific immunity can be achieved in one of two ways — through illness or vaccination. Since illness could lead to severe disease or death, vaccination is a better alternative as long as safe and effective vaccines can be developed.
How long before a coronavirus vaccine takes effect?
Generally speaking, it takes a week or two for immunity to develop following vaccination, but the specific timeline for any coronavirus vaccine will depend to some extent on which type of vaccine is licensed. For example, a live, weakened vaccine requires time to reproduce in the body, whereas an inactivated vaccine is given at a dose that will generate immunity. On the other hand, because the live, weakened vaccine reproduces to generate immunity, it might provide a more robust immune response than an inactivated vaccine
Bad Weather Brings Flu – Makes Sense
By Shlomo Maital
The conflation of COVID-19 and the fall/winter influenza season worries public health officials. In Israel, hospitals are already over-stretched – and doctors and nurses dread the onslaught of flu patients, on top of several thousand new COVID-19 cases daily. This is why Israel is now in partial lockdown, during the High Holydays.
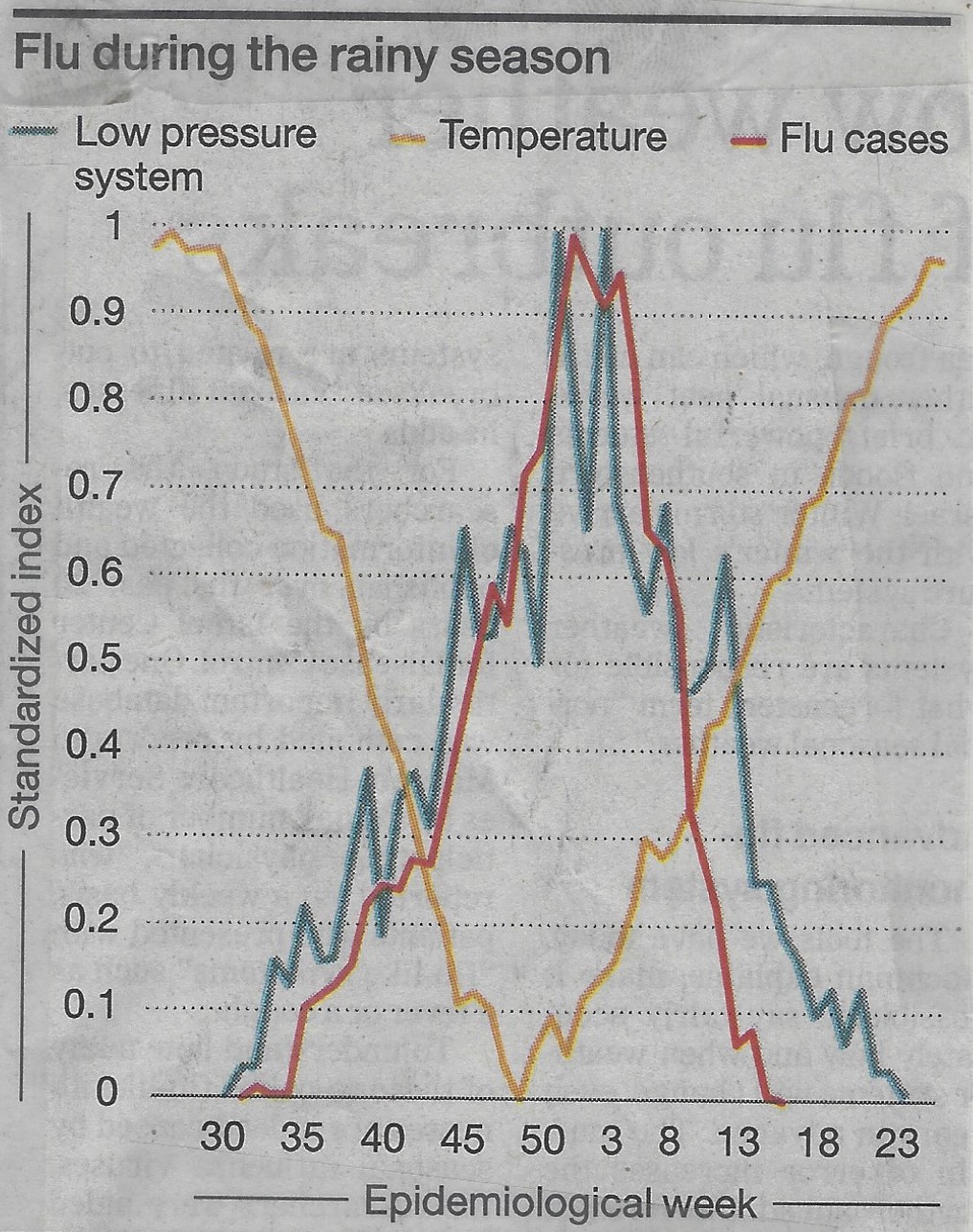
A new study by a group of Israeli and Mideast scholars shows, for the Eastern Mediterranean, a close correlation between climate and flu. *
The orange line above shows temperature. The red line: % of the population with flu. And the blue line: barometric pressure (inverted – high scale means low pressure). All three variables have been converted to a standardized zero to one normalized scale.
So – what is the connection between weather and flu?
It is pretty simple. Flu spreads through contact from one person to another. Outdoors, winds, even light breezes, disperse flu particles from sneezes and coughs and breathing. Indoors, this is far less true. In bad weather, people spend more time indoors. Hence, more flu.
This finding seems relevant for COVID-19 too. A friend of mine, a veteran pulmonary medical specialist, observes:
“With each cough and sneeze, there are very small particles under 10 microns in diameter, especially those under 2.5 microns, that tend to remain suspended in the air for a long time. This aerosol is scattered all over. While the volume of these particles is low, their surface area is large and lots of virus particles can stick to the surface of these small particles. It is now fully accepted that the virus’ transmission by aerosols is an important vector. The relatively large area of the eyes’ surface makes them vulnerable to the landing and culture of viruses. Protection against sprays and eye protection are crucial to creating barriers against contracting COVID-19.”
“Cough is the dominant mode of spread and as such should be monitored in areas where people congregate to assess risk in an objective mode and to identify possible spreaders. Cough monitoring is feasible with devices being available and used in pulmonary and occupational contexts.”
“The dilution in open air is immense. Consider the following example: A soft wind is blowing at 3.6 km/hour (2.2 miles per hour). If we consider a 4-meter- long test volume of air, the flow of air in the wind will sweep the test volume in four seconds, or nearly a thousand times per hour. This is significant and should be sufficient to prevent infection if very sporadic individuals are present. But if a distance of two meters cannot be observed at all times, the risk level is such that the use of a mask, at least surgical or cloth, is still required in the open.”
So, the message here is clear. We MUST get this second wave of COVID-19 under control before the flu season. If we don’t we will have two problems:
- Bad weather will bring influenza, and some flu sufferers will need hospitalization
- Bad weather will send people indoors, and COVID-19 spreads more easily there.
Hochman, A., Alpert, P., Negev, M., Abdeen, Z., Abdeen, A. M., Pinto, J. G., & Levine, H. (2020). The relationship between cyclonic weather regimes and seasonal influenza over the Eastern Mediterranean. Science of The Total Environment, 141686.
Is COVID-19 Mutating? Yes – But Not Harmfully!
By Shlomo Maital
I’ve been worrying about whether the SARS-CoV-2 virus (the piece of RNA that gives people COVID-19) is mutating. Evolution is everywhere and inexorable, and it creates animals, insects and even viruses that are well adapted to survive and meet threats. So, I wondered, is the novel coronavirus mutating, to defeat our best efforts?
The answer is no. Here are answers from Dr. Edward Holmes, an evolutionary virologist at University of Sydney, in today’s New York Times.* I present his findings as Q&A:
- “The coronavirus is mutating, and that’s fine (so far).” NYT Sept. 14, p. 11.
Do viruses really mutate?
“Viruses routinely mutate — and most of these changes are bad for the virus or even fatal, according to some studies. (A minority of mutations are neutral, and only a tiny minority beneficial.) The word “mutation” may sound ominous, but it is a humdrum fact of viral life and its implications most often aren’t nefarious for humans.”
Has COVID-19 become more virulent, more dangerous?
“ The real question is this: Has it become more virulent or more infectious than it was when it was first detected in Wuhan, central China, in December? The evidence suggests that it has not. Like the viruses that give us influenza or measles, SARS-CoV-2 has a genetic code made up of RNA, or ribonucleic acid. But RNA is highly mutable, and since SARS-CoV-2 infects us by using our body’s cells to replicate itself again and again, every time its genome is copied, an error might creep in. Most mutations are quickly lost, either by chance or because they damage some part of the virus’s main functions. Only a small proportion end up spreading widely or lasting. Mutation may be the fuel of evolution but, especially for an RNA virus, it also is just business as usual.”
How fast is COVID-19 mutating?
“RNA viruses tend to evolve rapidly — about a million times faster than human genes. Yet if SARS-CoV-2 stands out among them, it is for evolving more slowly than many: about five times less rapidly than the influenza viruses, for example. According to Nextstrain, an open-source project that tracks the evolution of pathogens in real time, and other sources, SARS-CoV-2 is accumulating an average of about two mutations per month — which means that the forms of the virus circulating today are only about 15 mutations or so different from the first version traced to the outbreak in Wuhan. To my knowledge, there is to date no evidence that SARS-CoV-2 has become more virulent or more lethal — nor, for that matter, that it has become less so.”
Even if COVID-19 has not mutated to a more dangerous form, that kills more people – has it perhaps mutated to become more infectious – in a way Nature often does, to reproduce better? Is THIS perhaps why the coronavirus has created strong second waves in many countries?
“I do not believe that the evolution of SARS-CoV-2 is what’s driving the virus’s continued spread. The coronavirus remains good at propagating itself because most of us still are susceptible to it; we are not immune, and it can still find new hosts to infect relatively easily.”
Are you sure?
“There has been much discussion over whether the D614G mutation — which affects the so-called spike protein of the virus — has made SARS-CoV-2 more infectious. The spike protein sits on the surface of the coronavirus, and it matters because it’s the part of the virus that attaches to the host’s cells. “D614G” is shorthand for a change at position 614 of the spike protein, from an aspartic acid (D) to a glycine amino acid (G). (The technical literature refers to “D614” as the earlier configuration and “G614” as the later one.) The D614G mutation, which probably initially arose in China, first appeared to become more and more frequent in the outbreak in northern Italy in February. The G614 form of the virus has since spread all over the world and has become the dominant variant. The D614G mutation does seem to have increased the infectivity of the coronavirus — at least in cells grown in laboratories, according to a recent paper by the computational biologist Bette Korber and others published in the journal Cell.”
“Apparently based partly on this and other studies, health authorities in various countries have claimed that the G614 form of the coronavirus may be 10 times more infectious than the version first detected in Wuhan. But as some epidemiologists have warned, it is difficult, not to mention unwise, to extrapolate from lab results to explain how the virus actually spreads in a real population. In the issue of Cell …. the viral epidemiologist Nathan Grubaugh and colleagues argued that the “increase in the frequency of G614 could be explained by chance and the epidemiology of the pandemic.”
Bottom line?
“For now, though, SARS-CoV-2 essentially is the same virus that emerged in December. Sure, it has mutated, but not, so far, in ways that should change how scientists think about how to tackle it — and not in ways that should worry you.”

