
You are currently browsing the tag archive for the ‘COVID-19’ tag.
The Race to a COVID-19 Vaccine: Q&A
By Shlomo Maital

Where do we stand in the quest for a safe effective COVID-19 vaccine?
More than 2.2 million persons worldwide have contracted the virus and of those, 154,783 have died. That is a 6.8% death rate. But wait – there are far far more cases worldwide than those we know about. Deaths are certain; cases are a guess. If we use a 1% to 1.5% death rate, we can guess that between 10 million and 15 million persons worldwide have contracted the illness. Only an effective vaccine will put a clear end to this crisis, in which COVID-19 is already the #1 cause of death in the US.
This Q&A is based on an informative survey published in a reputable website, livescience.com, by staff writer By Nicoletta Lanese, two days ago: (Warning: this blog is long, 1895 words…sorry).
* https://www.livescience.com/coronavirus-covid-19-vaccine-timeline.html
When will a vaccine be ready?
“Here’s why it probably can’t be developed any sooner than 12 to 18 months.
“More than 60 candidate vaccines are now in development, worldwide, and several have entered early clinical trials in human volunteers, according to the Some groups aim to provoke an immune response in vaccinated people by introducing a weakened or dead SARS-CoV-2 virus, or pieces of the virus, into their bodies. The vaccines for measles, influenza, hepatitis B and the vaccinia virus, which causes smallpox, use these approaches, according to the U.S. Department of Health & Human Services. Although tried-and-tested, using this approach to develop these conventional vaccines was labor-intensive, requiring scientists to isolate, culture and modify live viruses in the lab.
That initial process of just creating a vaccine can take 3 to 6 months, “if you have a good animal model to test your product,” Raul Andino-Pavlovsky, a professor in the Department of Microbiology and Immunology at the University of California, San Francisco, told Live Science. “
Are there short cuts? How fast is the US working on a vaccine?
“The first COVID-19 vaccine to enter clinical trials in the United States, for example, uses a genetic molecule called mRNA as its base. Scientists generate the mRNA in the lab and, rather than directly injecting SARS-CoV-2 into patients, instead introduce this mRNA. By design, the vaccine should prompt human cells to build proteins found on the virus’ surface and thus trigger a protective immune response against the coronavirus. Other groups aim to use related genetic material, including RNA and DNA, to build similar vaccines that would interfere with an earlier step in the protein construction process. But there’s one big hurdle for mRNA vaccines. We can’t be sure they will work. As of yet, no vaccine built from a germs’ genetic material has ever earned approval, Bert Jacobs, a professor of virology at Arizona State University and member of the ASU Biodesign Institute’s Center for Immunotherapy, Vaccines and Virotherapy, told Live Science. Despite the technology having existed for almost 30 years, RNA and DNA vaccines have not yet matched the protective power of existing vaccines, National Geographic reported.
In this high-stakes competition, is there also collaboration?
“Assuming these unconventional COVID-19 vaccines pass initial safety tests, “will there be efficacy?” Jacobs said. “The animal models suggest it, but we’ll have to wait and see.” “Because of the emergency here, people are going to try many different solutions in parallel,” Andino-Pavlovsky said. The key to trialing many vaccine candidates at once will be to share data openly between research groups, in order to identify promising products as soon as possible, he said.
Could a COVID-19 vaccine be potentially dangerous and do damage?
For sure.
“Designing a vaccine that grants immunity and causes minimal side effects is no simple task. A coronavirus vaccine, in particular, poses its own unique challenges. Although scientists did create candidate vaccines for the coronaviruses SARS-CoV and MERS-CoV, these did not exit clinical trials or enter public use, partly because of lack of resources, Live Science previously reported. “One of the things you have to be careful of when you’re dealing with a coronavirus is the possibility of enhancement,” Fauci said in an interview with the journal JAMA on April 8. Some vaccines cause a dangerous phenomenon known as antibody dependent enhancement (AED), which paradoxically leaves the body more vulnerable to severe illness after inoculation. Candidate vaccines for dengue virus, for example, have generated low levels of antibodies that guide the virus to vulnerable cells, rather than destroying the pathogen on sight, Stat News reported. Coronavirus vaccines for animal diseases and the human illness SARS triggered similar effects in animals, so there’s some concern that a candidate vaccine for SARS-CoV-2 might do the same, according to an opinion piece published March 16 in the journal Nature. Scientists should watch for signs of AED in all upcoming COVID-19 vaccine trials, Fauci said. Determining whether enhancement is occurring could happen during initial animal studies, but “it is still unclear how we will look for AED,” Jacobs said.
Are there specific dangers in developing a COVID-19 vaccine?
A successful coronavirus vaccine will snuff the spread of SARS-CoV-2 by reducing the number of new people infected, Andino-Pavlovsky said. COVID-19 infections typically take hold in so-called mucosal tissues that line the upper respiratory tract, and to effectively prevent viral spread, “you need to have immunity at the site of infection, in the nose, in the upper respiratory tract,” he said. These initial hotspots of infection are easily permeated by infectious pathogens. A specialized fleet of immune cells, separate from those that patrol tissues throughout the body, are responsible for protecting these vulnerable tissues. The immune cells that protect mucosal tissue are generated by cells called lymphocytes that remain nearby, according to the textbook “Immunobiology: The Immune System in Health and Disease” (Garland Science, 2001).
“It’s like your local police department,” Andino-Pavlovsky told Live Science. But not all vaccines prompt a strong response from the mucosal immune system, he said. The seasonal influenza vaccine, for example, does not reliably trigger a mucosal immune response in all patients, which partly explains why some people still catch the respiratory disease after being vaccinated, he said.
“Even if a COVID-19 vaccine can jumpstart the necessary immune response, researchers aren’t sure how long that immunity might last, Jacobs added. While research suggests that the coronavirus doesn’t mutate quickly, “we have seasonal coronaviruses that come, year in [and] year out, and they don’t change much year to year,” he said. Despite hardly changing form, the four coronaviruses that cause the common cold keep infecting people — so why haven’t we built up immunity?
Could the COVID-19 virus pose special problems?
“Perhaps, there’s something odd about the virus itself, specifically in its antigens, viral proteins that can be recognized by the immune system, and that causes immunity to wear off. Alternatively, coronaviruses may somehow fiddle with the immune system itself, and that could explain the drop-off in immunity over time, Andino-Pavlovsky said. To ensure a vaccine can grant long-term immunity against SARS-CoV-2, scientists will have to address these questions. In the short term, they’ll have to design experiments to challenge the immune system after vaccination and test its resilience through time, Jacobs said. In a mouse model, such studies could take “at least a couple of months,” he said. Scientists cannot conduct an equivalent experiment in humans, but can instead compare natural infection rates in vaccinated people to those of unvaccinated people in a long-term study. “When you have the luxury, you look at this for five years, 10 years to see what happens,” Andino-Pavlovsky added.
How will they ensure that a COVID-19 vaccine is safe?
“Unlike an antiviral treatment for COVID-19 that can be given to patients already infected with the virus, a vaccine must be tested in diverse populations of healthy people. “Because you give it to healthy people, there’s an enormous pressure to make sure it’s absolutely safe,” Andino-Pavlovsky said. What’s more, the vaccine must work well for people of many ages, including the elderly, whose weakened immune systems place them at heightened risk of serious COVID-19 infection. “Initially, safety studies will be done in small numbers of people,” likely fewer than 100, Jacobs said. A vaccine may be approved based on these small studies, which can take place over a few months, and then continually monitored as larger populations become vaccinated, he added. “That’s just my guess.”
[Note: The high and growing death toll from COVID-19 may justify some speed-up and short-cuts].
So what are the various stages that a vaccine must undergo, before it can be mass produced?
“Any potential vaccine will need to pass a safety trial, known as a Phase 1 trial, which also helps determine the needed dose. The next step is a larger trial in 100 to 300 people, called a Phase 2, which looks for some biological activity, but can’t say for sure if the drug is effective. If a vaccine candidate prompts a promising immune response in Phase 2 clinical trials, after passing safety tests in Phase 1, it’s possible that the FDA could approve such a vaccine for emergency use “before the 18-month period that I said,” Fauci said in the JAMA interview. “If you get neutralizing antibodies,” which latch onto specific structures on the virus and neutralize it, “I think you can keep moving forward on it,” Jacobs said. Normally, a vaccine would then enter Phase 3 clinical trials, which include hundreds to thousands of people.
“So adding up these steps, each of which will likely take 3 to 6 months, it’s very unlikely we would be able to find a vaccine that is safe and effective in less than 12 months — even if many of these steps could be done in parallel.
Can it be mass-produced? How?
“Then comes the issue of manufacturing billions and billions of doses of a new vaccine whose ingredients we don’t yet know. Bill Gates has said that the Gates Foundation will fund the construction of factories for seven coronavirus vaccine candidates, equipping the sites to produce a wide variety of vaccine types, Business Insider reported.
[Neanderthal Conservative groups have attacked Gates, making false and inflammatory claims about him].
“Even though we’ll end up picking at most two of them, we’re going to fund factories for all seven, just so that we don’t waste time in serially saying, ‘OK, which vaccine works?’ and then building the factory,” Gates said. Even if a fairly promising vaccine surfaces by 2021, and can be mass-produced, the search won’t end there. “Especially with trying to get something out this quickly, we may not get the best vaccine out there right away,” Jacobs said. Ideally, an initial vaccine will grant immunity for at least one to two years, but should that immunity wane, a longer lasting vaccine may have to be deployed. Historically, so-called live attenuated vaccines that contain a weakened virus tend to perform most reliably over extended periods of time, Andino-Pavlovsky said.
“That may be what we need in the long run,” he said. And research into coronavirus immunity should continue, regardless, “not only for COVID-19, but for the next coronavirus that comes.
Remdesivir: Grasping at Straws!
By Shlomo Maital

There is a massive amount of fake news circulating now about COVID-19, some of it racist, pernicious and dangerous. There is also well-meaning news, reports that want to bring hope but in fact are simply grasping at straws.
A report now viral, emanating from the University of Chicago, is about how an anti-viral drug developed by a pharma company, Gilead, has helped seriously ill COVID-19 patients.
Remdesivir is an antiviral medication; a nucleotide analog, specifically an adenosine analogue, which inserts into viral RNA chains, causing their premature termination. It is being studied during 2020 as a possible post-infection treatment for COVID-19 illness.
A U of Chicago doctor participated in an internal hospital video in which she reported that when seriously ill patients administered remdesivir, many recovered.
The video reached some hospital employees, who leaked it to journalists. That led to a highly optimistic report.
This is not a clinical test. There is no protocol, and no placebo (sugar pill given to some patients).
The drug, made by Gilead Sciences, was tested against Ebola with little success, but multiple studies in animals showed the drug could both prevent and treat coronaviruses related to Covid-19, including SARS (Severe Acute Respiratory Syndrome) and MERS (Middle East Respiratory Syndrome).
We are all desperate for some good news. But grasping at straws is not going to help. The journalists who reported this “scoop” should have told us exactly what the source was, an internal chatty ‘gossip’ video of the kind that circulates in most hospitals.
The journalist who DID inform us was the CNN medical correspondent, is Elizabeth Cohen, who has serious training and deep scientific knowledge. She has a Master’s degree in public health. Her colleague is Dr. Sanjay Gupta, a neurosurgeon; together they comprise “the horse’s mouth” and to mix a metaphor, a horse’s mouth that does NOT grasp at straws.
Does the Novel Coronavirus Mutate?
By Shlomo Maital

Writing in today’s New York Times, Nathaniel Lash and Tala Schlossberg try to answer the key question, does the novel coronavirus mutate? If so, how and when?
Here is why it is important for us to know this. The pandemic crisis will end only when we have a vaccine, produced in billions of doses. The vaccine will work by stimulating the body to produce antibodies that neutralize the virus by binding to it in a very specific way. If the virus can mutate to defeat the vaccine, then the vaccine will not stop working. The key is the “spike protein” – the protein the virus makes that penetrates the cell walls and lets the virus invade (and kill) it. Those are the spikes you see in the graphic illustrations of corona. Vaccines can defeat the spike.
Here is what the authors of the article have found:
“Among the thousands of samples of the long strand of RNA that makes up the coronavirus, 11 mutations have become fairly common. But as far as we know, it’s the same virus infecting people all over the world, meaning that only one “strain” of the virus exists, said Peter Thielen, a molecular biologist with the Johns Hopkins Applied Physics Laboratory. Only one of those common mutations affects the “spike protein,” which enables the virus to infect cells in the throat and lungs. Efforts to produce antibodies that block the spike protein are central to many efforts to develop a vaccine. Since the spike protein has changed little so far, some scientists believe that’s a sign that it can’t alter itself very much and remain infectious.”
So – we have a small piece of good news. The measles vaccine, for instance, was developed in 1950. And it is still effective. Measles hasn’t mutated in a manner that neutralizes the vaccine. Evolution is powerful – but apparently it cannot surmount EVERY obstacle. So hopefully the same will apply to the COVID-19 vaccine – and we will bid this insidious deadly enemy good-bye, with an effective vaccine… until the next one.
Viral Shedding Peaks – BEFORE Symptoms!
By Shlomo Maital

The late Li Wenliang, China’s hero doctor who warned us
A very large number of research papers are now emerging from China, by Chinese scientists and scholars, related to biology, medicine, education, and other areas. China is sharing with the world what it has learned.
Yesterday’s Nature Medicine features a very important article by a large group of Chinese researchers, which shows this:
“We report temporal patterns of viral shedding in 94 patients with laboratory-confirmed COVID-19 and modeled COVID-19 infectiousness profiles from a separate sample of 77 infector–infectee transmission pairs.
We observed the highest viral load in throat swabs at the time of symptom onset, and inferred that infectiousness peaked on or before symptom onset. We estimated that 44% (95% confidence interval, 25–69%) of secondary cases were infected during the index cases’ pre-symptomatic stage, in settings with substantial household clustering, active case finding and quarantine outside the home. Disease control measures should be adjusted to account for probable substantial presymptomatic transmission.”
Meaning? Three rather scary words: substantial pre-symptomatic transmission. We spread the coronavirus even before we feel symptoms.
This is why social distancing will need to be enforced for quite some time, until tests are widely available and can provide results within hours. If you have no symptoms, then anybody can be a carrier and spreader. Anybody.
Finally, we are learning about this insidious enemy – is anyone expressing some gratitude to the Chinese for sharing?
Well, a small gesture – here are the names of the researchers who co-authored this paper: Xi He, Eric H. Y. Lau, Peng Wu, Xilong Deng, Jian Wang, Xinxin Hao, Yiu Chung Lau, Jessica Y. Wong, Yujuan Guan, Xinghua Tan, Xiaoneng Mo, Yanqing Chen, Baolin Liao, Weilie Chen, Fengyu Hu, Qing Zhang, Mingqiu Zhong, Yanrong Wu, Lingzhai Zhao, Fuchun Zhang, Benjamin J. Cowling, Fang Li & Gabriel M. Leung
A Vaccine is Coming – from Pittsburgh
By Shlomo Maital

Univ. of Pittsburgh “Cathedral of Learning”
Before the good news about a COVID-19 vaccine – a piece of history.
In 1947, native New Yorker Jonas Salk accepted an appointment to the University of Pittsburgh School of Medicine. In 1948, he undertook a project funded by the National Foundation for Infantile Paralysis to determine the number of different types of poliovirus. Salk saw this was a golden opportunity to extend this project towards developing a vaccine against polio. He built a research team and devoted himself to this work for the next seven years. The field trial set up to test the Salk vaccine involved 20,000 physicians and public health officers, 64,000 school personnel, and 220,000 volunteers. Over 1.8 million schoolchildren took part in the trial.
On March 26, 1953, Salk announced on a national radio show that he had successfully tested a vaccine against poliomyelitis, the virus that causes the crippling disease of polio. In 1952—an epidemic year for polio—there were 58,000 new cases reported in the United States, and more than 3,000 died from the disease. Dr. Salk was celebrated as the great doctor-benefactor of his time.
Fast forward. A press release from the NIH: https://www.nih.gov/news-events/nih-research-matters/microneedle-coronavirus-vaccine-triggers-immune-response-mice
“After the identification of SARS-CoV-2, the genome sequence of the new coronavirus was rapidly released to the public by scientists in China. Several weeks later, National Institute of Health-funded scientists produced a detailed picture of the part of the virus, called the spike protein, that allows it to infect human cells. This spike protein is currently the target of several vaccine development efforts. And we see the graphic version of the corona ‘spikes’ everywhere…
“Researchers led by Drs. Louis Falo, Jr. and Andrea Gambotto from the University of Pittsburgh have been working to develop vaccines for other coronaviruses, including the one that causes Middle East Respiratory System (MERS). They adapted the system they had been developing to produce a candidate MERS vaccine to rapidly produce an experimental vaccine using the SARS-CoV-2 spike protein.
The team developed a method for delivering their MERS vaccine into mice using a microneedle patch. Such patches resemble a piece of Velcro, with hundreds of tiny microneedles made of sugar. The needles prick just into the skin and quickly dissolve, releasing the vaccine. Since the immune system is highly active in the skin, delivering vaccines this way may produce a more rapid and robust immune response than standard injections under the skin.
“When delivered by microneedle patch to mice, three different experimental MERS vaccines induced the production of antibodies against the virus. These responses were stronger than the responses generated by regular injection of one of the vaccines along with a powerful immune stimulant (an adjuvant). Antibody levels continued to increase over time in mice vaccinated by microneedle patch—up to 55 weeks, when the experiments ended.
“Using knowledge gained from development of the MERS vaccine, the team made a similar microneedle vaccine targeting the spike protein of SARS-CoV-2. The vaccine prompted robust antibody production in the mice within two weeks.
“The vaccinated animals haven’t been tracked for enough time to see if the long-term immune response is equivalent to that observed with the MERS vaccines. The mice have also not yet been challenged with SARS-CoV-2 infection. However, the findings are promising in light of results from the similar MERS vaccine.
“The components of the experimental vaccine could be made quickly and at large-scale, the researchers say. The final product also doesn’t require refrigeration, so it could be produced and placed in storage until needed. The team has now begun the process of obtaining approval from the U.S. Food and Drug Administration to launch a phase 1 trial within the next several months.
“Much work still needs to be done to explore the safety and efficacy of this candidate vaccine. “Testing in patients would typically require at least a year and probably longer,” Falo says. “This particular situation is different from anything we’ve ever seen, so we don’t know how long the clinical development process will take.”
OK – it works in mice. Now for humans. A vaccine is on the way – and it may emerge again from Univ. of Pittsburgh.
How to Emerge from Lockdown: Speed is Vital!
By Shlomo Maital
Question: how does coronavirus resemble standup comedy?
Answer: For both, timing is crucial.
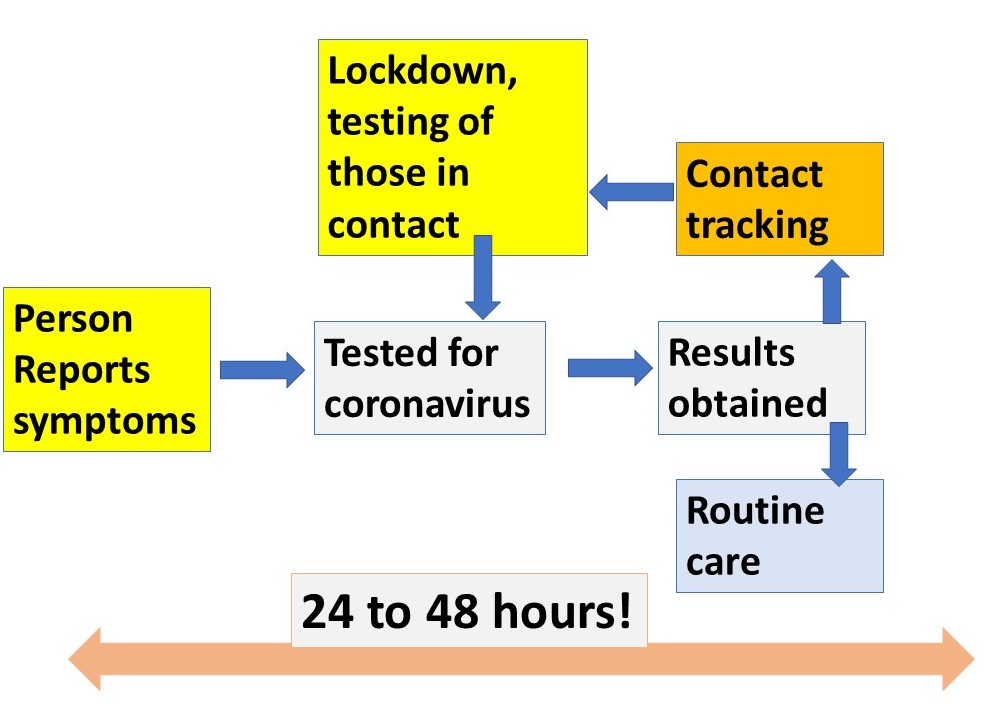
As countries begin to emerge from lockdown (Denmark has opened its kindergartens, because 90% of families with children have both parents working), fears arise whether this is wise. One answer is, yes, but… The diagram above shows how emergence can best be done. And everything, EVERYthing, depends on timing and speed —
- test for virus among those with symptoms, and some who are asymptomatic,
- get the results super-fast, within hours (this is possible with some tests),
- track those in contact with persons testing positive,
- lock down those with the virus, and
- do this again and again.
All this depends on revising current testing procedures (some results have been lost, some take 6-8 days for results, far too long to be useful). Timing and speed are crucial. Why? Because, in the 6 days it takes now for results to be provided, the person potentially infected can infect many many other people, even unknowingly.
Does your country have test results within minutes or even hours? There are such tests. We need millions of them.
What Do We NOT Know?!
By Shlomo Maital

After more than four months of nonstop news/debate/discussion around COVID-19, it is astonishing how much we do not know. And as the saying goes, what you don’t know that you don’t know — is the worst; it can literally kill you.
So here is my attempt to list, what it is we don’t know, that we NEED to know, about this tiny virulent enemy and hopefully, scientists are working on it.
- For those who get COVID-19 and recover, are they immune? For life? For a short time? How long does the immunity last?
- Like many viruses, can this novel coronavirus mutate quickly and attack those who contracted an older version? Are COVID-19 cases in the US characterized by the same genetically-identical virus as say in China, or different? If so, how different? And does it matter?
- Intubation: Are we in too much of a hurry to put people on intubation (ventilators)? If such a small percentage of those intubated, survive, should we rethink this? And how different are the various kinds of ventilators (those used by anesthetists, oxygen ventilators, standard ventilators, etc.)?
- Why are the death rates (those who die from COVID-19, as a % of those who are seriously ill, or in general % of those who contract the virus) different, radically, between one country and another? How much of this is due to ICU expertise?
- How exactly does COVID-19 spread? As aerosol (tiny droplets that hang in the air for hours?) As big droplets (that fall to the ground fairly quickly)?
- Are there drugs proven to be effective against COVID-19? What about the recently-approved anti-influenza drugs? Xofluza, Tamiflu, Relenza, Rapivab ? And, of course, hydroxychloroquine? (which seems to have severe heart side-effects among some patients).
- Why are African-Americans more afflicted than Caucasians? Men more than women?
- Will there be a second wave? And a third? How will we know in time?
- How soon will we have a proven vaccine, and how quickly can doses be produced, to inoculate billions of people? How much will it cost? Can it be provided for free? How can the many companies working on a vaccine, in many countries, work together, to save time and save lives?
- What countries have managed the COVID-19 crisis best, and what can be learned from them? There have been many variations on lockdown, ranging from easy (Sweden) to draconian (China, Singapore). Which works best?
- Somewhere, as we speak, a new virus is brewing and mutating somewhere; this is not the last pandemic. Can we organize a world-spanning organization (broader in span than WHO, with far more resources) that will be ready to tackle the next pandemic quickly and efficiently? With massive resources?
I’m certain there are a thousand more things we do not know. Add your own questions… for each question above, there are multiple answers online, and many of them are fake or conspiratorial. This simply adds to the fog.
Political Leaders: Step Back! Let the Pros Do It!
By Shlomo Maital

Ladies and gentlemen, golf fans! Here we are, on the 18th green, at the legendary Master’s tournament. Byron Putput has a 30-foot put for birdie, to win the Green Jacket and the championship. He’s thinking. He’s looking. He’s planning… all his 24 years of golfing are going into this crucial put! The fans are silent. The tension is palpable.
But wait. Here comes… Donald Trump. Yes, Donald Trump. POTUS, he’s called, President of the United States. Yes, fans, he is shoving aside Byron. Executive privilege, he says. Trump himself will take the put. He pulls a putter out of the golf bag – but wait, it is not a putter, but an iron. He’s going to do the put with an iron!
Oh my gosh. Is this really happening?
……. No, it’s not. Or is it? Reopening the US economy is, “I would say, without a doubt, that it is the most important decision I have ever had to make,” Trump said three days ago. First person singular. I. Not ‘we’. And he doesn’t even have the authority to decide, it is really up to the state governors.
Let’s make some sense out of this. Giora Eiland is Major General (ret.) Israel Defense Forces. Eiland is a former head of the Israeli National Security Council. Speaking on Israeli Radio, he made this point:
In the pandemic, Israel (and every country) is at war. This requires mobilization of all our energy, skills, wisdom and resources. Israel has done this, alas, numerous times in the past. But how? As we do in wartime, as US and UK did in wartime. Set up a panel of experts. NOT politicians! In health, economy, education, psychology, science, medicine. Put them in a room. Let them define the issues, then divide up according to “comparative advantage” and work out alternatives and plans. Nonstop. Round the clock. Sleep on cots in the room or nearby.
Israel’s Ministry of Health has disastrously mismanaged the issue of performing COVID-19 testing. And testing, by all experts, is key to emerging from quarantine. The IDF (army) could have done it faster, better, more professionally. But internal political squabbles between Israel’s Prime Minister and the Defense Minister (whom the PM hates), Netanyahu’s nemesis, prevented this. Too bad. We are paying the price today.
Trump will not take the final put at the Master’s golf tournament. A pro golfer will do that. Why are we letting him, or Netanyahu, or Macron, or Johnson, take the lead in managing the epidemic? Step back politicians. Step aside. Let the professionals manage this war. Because you politicians do not have a clue.
One possible exception: NY State Governor Andrew Cuomo. In his amazing daily briefings, he shows a wonderful grasp of data, curves, expert opinion, trends, and illustrates his talks with informative slides and graphs. But this exception proves the rule.
Learn from Spain:
We WILL Err – but how?

By Shlomo Maital
Spain has suffered terribly from the new coronavirus. The numbers tell the tale:
Cases overview
Spain
| Confirmed
169,496 |
Recovered
64,727 |
Deaths
17,489 |
For a nation of 47 million, this is a terrible toll. It is explained in part by Spain’s late start in lockdown, and its Mediterranean open lifestyle, in the cafes and markets, during a warm spring.
But it seems to have peaked. The number of new cases peaked in Spain, at 8,000, daily, on April 2, and has now declined to about 4,000. So Spain is gradually beginning to emerge from lockdown, to revive the economy, in a planned careful and staged manner.
I think other countries should watch Spain carefully, talk to Spanish experts, learn about their plan, adapt the plan to their own nations’ needs and nature…and in general, we need a global brainstorming conference. An international Zoom of experts.
Take Korea. There has been a resurgence, there, a second wave, but not huge, 100 cases. OK – what happened? Is the immunity conferred by having the COVID-19 and recovering from it sufficient to give permanent immunity? Or can a huge dose of the virus come back and attack you again? Let’s find out from Korea.
How is Singapore handling the ‘track down those who spread it’? We will need to have a system for that, when we (many of us) return to work.
We should have a website clearing house for things countries have learned, but a credible one, with only vetted proven entries by real experts.
What do we know about this vicious viral enemy? Can we compile a COVID-19 handbook – here is what we know, and how we know it, and what the source of the data is.
And regarding emerging from the ‘shelter at home’ lockdown — Trump says this is the most important decision of his life. HIS decision? If I were an American, would I feel reassured in having TRUMP???? make the decision? When his ‘base’ is calling for the resignation of Fauci, a credible epidemiology expert, who urges caution?
We will make mistakes and already have. Trump’s January-February fumbling cost many lives. Maybe, it is best to err on the side of caution, as we emerge from lockdown. Let’s study Spain carefully.
Rule of 72: One More Time
By Shlomo Maital
Sorry, but – one more time for the Rule of 72. Many print and cable journalists are rather innumerate – they took Philosophy 1 instead of Calculus 1 in college. So it is no wonder they struggle to interpret the COVID-19 numbers for us, and simply throw totals at us, without really explaining what they mean. So, it’s left to us citizens to “do the math”. And, alas, that math could involve logarithms.
(Someone I know well, recently asked me, is a logarithm the same as an algorithm? Because, high school teachers themselves don’t seem to know what logarithms) are).
So, first, a quibble. CNN, when you show your COVID-19 graphs, daily numbers, can you please do it on a logarithmic scale, not absolute numbers? (in Excel, you can use the log( ) function or the ln ( ) function, where ln is the log to base ‘e’ 2.71828 and log is the log to the base 10… ok, never mind about all that! But the reason for logs is, the steepness of the logarithmic curve shows the rate of change, and you can easily tell if the curve is getting steeper (rate of change is rising) or less steep (rate of change is slowing), and this is of course CRUCIAL!).
So, some of you, maybe very few, maybe VERY VERY few, want to know, where does this Rule of 72 come from? (Divide 72 by the daily rate of change of COVID-19 patients, and you get the number of days it takes for the number of those infected to double). If it’s 10%, it doubles every week – disaster. If it’s 2%, it doubles every 36 days, about monthly – phew…we made it.
So here is the basic equation:
(1+R/100)T = 2
Where R is the rate of (daily) change, in %, T is the number of days it takes to double, and 2, well, that’s the doubling, e.g. a 10% daily spread rate will double in 7 days: (1+0.1)7 = 2
If you take the logarithm of each side of the equation, you get this:
T ln(1+R/100) = ln 2 (trust me!)
So T, the number of days it takes for the virus to double the number infected, if the rate of spread growth is R, is equal to
T = ln2 / ln(1+R/100)
Now, mathematicians pull a neat trick out of their bag of tricks, and find a way to simplify this equation, so we don’t need calculators or log tables:
T = 72/R
Hence Rule of 72: divide 72 by the rate of spread, you get ‘days to double’. (One last word, skip this is you wish — you can do this approximation using a neat way to find approximations called a Taylor Function, neatly tailored by mathematicians to simplify our lives…).
Normally, we use Rule of 72 to see how many years it will take for our money to double. Well-heeled people get 8% interest on their money, or more, usually through the stock market, so their millions double on their own every 72/8 = 9 years.
Initially the virus was spreading at 25% growth rates daily, in many places, meaning the numbers infected were doubling every 72/25 = 3 days! Roughly. Yikes. Say 100 people were infected initially. At this rate, in 30 days, there will be 10 doublings. 10 doublings is 2 times 2 times 2, ten times, or 1,024. So those 100 infected become 100 x 1,000 or 100,000! THIS is why it was so absolutely crucial to jump on things early and lock everyone down. Alas, the US failed to do this. So did other nations.
So if TV and media fail to use Rule of 72 – do it yourself. Figure out the daily % rate of change of those infected with virus (come on, you can do it…. Today’s number / Yesterday’s number, minus 1 and then times 100. Then divide 72 by this number. Presto: Days to double. Big number? Worry. Small number? Yeah!

