
You are currently browsing the tag archive for the ‘vaccine’ tag.
Two Turks and a Greek Collaborate – And Save the World
By Shlomo Maital

Dr. Uğur Şahin and Dr. Özlem Türeci
Every major nation in the world is feverishly working to develop a vaccine against COVID-19. Billions of dollars have been spent, thousands enlisted, politics pollutes science — and in the end, the world will be saved by two brilliant people whose families emigrated from Turkey to Germany, together with a Greek CEO. Here is the story, based on David Gelles’ New York Times article.*
*David Gelles. They’re first in the face for a vaccine. NYT, Friday Nov. 13, 2020, p. 8
On Monday Nov. 9, Pfizer announced that a COVID-19 vaccine developed by Dr. Ugur Sahin and Dr. Ozlem Tureci had been shown to be over 90% effective. Predictably, Trump claimed falsely that the announcement had been purposely delayed to harm his re-election. The announcement was made by Albert Bourla, Pfizer CEO, who is Greek. What lovely irony that two Turks and a Greek combine to save the world!
Who are Ugur Sahin and Ozlem Tureci?
Sahin, 55, was born in Iskendurun, Turkey. His family moved to Cologne, Germany, when he was 4; his parents worked in a Ford car factory there. He graduated from the Univ. of Cologne as a medical doctor and later, Ph.D., after researching immunotherapy for caner. He met Dr. Tureci, 53, early in his career; she hoped to become a nun, but ended up studying medicine; she was the daughter of a Turkish physician who emigrated to Germany from Istanbul.
In 2001 Sahin and Tureci founded Ganymet Pharmaceuticals to develop monoclonal antibodies to treat cancer. [A monoclonal antibody is made by cloning a unique white blood cell, that bind to an antigen, e.g., a virus, cancer cell or bacteria and keep it from making us ill]. They sold Ganymet for $1.4 billion in 2016.
As billionaires, did they go off to bask on a beach in the Bahamas?
Far from it. They founded BioNTech, even before selling Ganymed, to use messenger RNA (mRNA) (see below) to treat cancer.
What insight did Dr. Sahin have two years ago?
At a conference in Berlin, Sahin told a roomful of infectious disease experts, that his company BioNTech “might be able to use messenger RNA to create a vaccine in the event of a global pandemic.” BioNTech began work on the vaccine in January, after Sahin read an article in a medical journal and saw how the novel coronavirus was about to spread worldwide. Scientists at BioNTech cancelled vacations and went to work on what they called Project Lightspeed (Trump copied Warpspeed from them).
What is an mRNA vaccine?
This is brand-new vaccine technology. “To produce an mRNA vaccine, scientists produce a synthetic version of the mRNA (RNA, ribonucleic acid, is a molecule vital in genetic coding and decoding) that a virus uses to build its infectious proteins. This mRNA is delivered into the human body, whose cells read it as instructions to build that viral protein, and therefore create some of the virus’s molecules themselves. These proteins are solitary, so they do not assemble to form a virus. The immune system then detects these viral proteins and starts to produce a defensive response to them.” This is a relatively new technology for creating vaccines. No such vaccine existed before.
What role does Pfizer play?
BioNTech developed the vaccine. But the process of clinical testing, passing regulation, and producing billions of doses, needed a Big Pharma company. BioNTech has been collaborating with Pfizer since 2018. Pfizer CEO Albert Bourla was born in Thessaloniki, Greece and has been with Pfizer since 1992. In March BioNTech and Pfizer signed a collaborative agreement.
Is BioNTech a major company?
It is now! Its market value has understandably soared, to over $21 billion, and it is based in Mainz, Germany, employing 1,323. This makes Sahin and Tureci among Germany’s wealthiest persons. However, they live in a modest apartment, with their teenage daughter, and bicycle to work. They do not own a car.
Will the BioNTech mRNA vaccine save the world?
Maybe. But a major problem will be transporting it. It requires cooling to minus 70 degrees C. Even major hospitals do not have storage facilities for a vaccine at that ultra-low temperature. The vaccine will have to be shipped in dry ice (solid frozen CO2), which is minus 78.5 degrees C.
COVID-19 Vaccines: What We Know
By Shlomo Maital

In my country Israel, there are more new daily cases per million population than anywhere in the world. Europe too is undergoing a second wave; and many states in the United States are also seeing increasing morbidity. So – everywhere, we await a vaccine.
Over a hundred different efforts are underway to create, produce and administer COVID-19 vaccines. Here is what we know so far, based on a very clear, lucid website sponsored by the Children’s Hospital of Philadelphia. This vaccine effort is an amazing global effort, led by the top scientific minds, trying a wide variety of creative approaches, some tried and true, some radical and innovative. One or more of them will save humanity!
What types of vaccine are being tested?
Several.
* Inactivated vaccine — The whole virus is killed with a chemical and used to make the vaccine. This is the same approach that is used to make the inactivated polio (shot), hepatitis A and rabies vaccines;
*Subunit vaccine — A piece of the virus that is important for immunity, like the spike protein of COVID-19, is used to make the vaccine. This is the same approach that is used to make the hepatitis and human papillomavirus vaccines.
* Weakened, live viral vaccine — The virus is grown in the lab in cells different from those it infects in people. As the virus gets better at growing in the lab, it becomes less capable of reproducing in people. The weakened virus is then used to make the vaccine. When the weakened virus is given to people, it can reproduce enough to generate an immune response, but not enough to make the person sick. This is the same approach that is used to make the measles, mumps, rubella, chickenpox and one of the rotavirus vaccines.
* Replicating viral vector vaccine — In this case, scientists take a virus that doesn’t cause disease in people (called a vector virus) and add a gene that codes for, in this case, the coronavirus spike protein. Genes are blueprints that tell cells how to make proteins. The spike protein of COVID-19 is important because it attaches the virus to cells. When the vaccine is given, the vector virus reproduces in cells and the immune system makes antibodies against its proteins, which now includes the COVID-19 spike protein. As a result, the antibodies directed against the spike protein will prevent COVID-19 from binding to cells, and, therefore, prevent infection. This is the same approach that was used to make the Ebola virus vaccine.
* Non-replicating viral vector vaccine — Similar to replicating viral vector vaccines, a gene is inserted into a vector virus, but the vector virus does not reproduce in the vaccine recipient. Although the virus can’t make all of the proteins it needs to reproduce itself, it can make some proteins, including the COVID-19 spike protein. No currently licensed vaccines use this approach.
* DNA vaccine — The gene that codes for the COVID-19 spike protein is inserted into a small, circular piece of DNA, called a plasmid. The plasmids are then injected as the vaccine. No currently licensed vaccines use this approach.
* mRNA vaccine — In this approach, the vaccine contains messenger RNA, called mRNA. mRNA is processed in cells to make proteins. Once the proteins are produced, the immune system will make a response against them to create immunity. In this case, the protein produced is the COVID-19 spike protein. No currently licensed vaccines use this approach.
Which type of COVID-19 vaccine is most likely to work?
It is likely that more than one of these approaches will work, but until large clinical trials are completed, we won’t know for sure. Likewise, the different approaches may have different strengths and weaknesses. For example, mRNA or DNA vaccines are much faster to produce, but neither has been used to successfully make a vaccine that has been used in people. On the other hand, killed viral vaccines and live, weakened viral vaccines have been used in people safely and effectively for many years, but they take longer to produce.
In addition to differences in how long it takes to make different types of vaccines, each type may also cause the immune system to respond differently. Understanding the immune responses that are generated will be important for determining whether additional (booster) doses will be needed, how long vaccine recipients will be protected, and if one type offers benefits over another.
Is one of the COVID-19 vaccines expected be more effective for the elderly population?
It is likely that COVID-19 vaccines could have different levels of effectiveness in various subgroups of people. Because the elderly generally do not respond as well to vaccines, one or more COVID-19 vaccines may not work well for them, which is concerning given their higher risk of severe disease. The large phase III studies may not include people over a certain age. But, the manufacturers have been encouraged to include older people, so that we have this type of information earlier in the process than may usually occur. We will have to wait and see what the data show to know which vaccine(s) work best in the older population.
How many doses of a COVID-19 vaccine will be needed? Will a booster dose be needed?
The number of doses of a COVID-19 vaccine that will be needed has not yet been determined. The coronavirus vaccines being studied are evaluating one or two doses. When giving two doses, they are usually given one or two months apart. We will need to wait for the results of the clinical trials to have more information about how many doses will be needed.
How long will vaccine immunity last?
Since we do not yet know how long immunity after infection lasts, immunity following vaccination will also have to be determined. Likewise, immunity following vaccination will depend in part on which types of vaccines are licensed, what part of the immune system responds to the vaccine, and the level of immunity that is generated by the vaccine.
If more than one vaccine becomes available, could taking two different vaccines boost the effectiveness?
While it is likely that more than one COVID-19 vaccine will become available, we probably won’t have a good answer to this question until vaccines are actually licensed and we know more about them. Three scenarios can occur if a person is vaccinated with two versions of vaccines against the same disease, particularly close in time:
— They get a stronger immune response. An example of this was when children got inactivated polio vaccine and later got oral polio vaccine.
—- The second vaccine causes immunity that would be similar to receiving a second dose of the original vaccine. Using a different brand of hepatitis B vaccine for one or more doses would be an example of this.
— The immune response generated by the first vaccine interferes with components of the response to the second vaccine, in some cases causing lower immunity. For example, when people got a pneumococcal polysaccharide vaccine (PPSV) followed by a pneumococcal polysaccharide vaccine with a harmless helper protein attached to it, called pneumococcal conjugate vaccine (PCV), they had lower antibody responses to one part of the PCV vaccine than people who got the two vaccines in the opposite order (PCV followed by PPSV).
For these reasons, studies will need to be done to determine the effects of getting a second type of COVID-19 vaccine shortly after receiving a different one. If, however, we find that COVID-19 vaccines are like influenza vaccines and we need to get vaccinated annually, concerns about switching types from one year to the next are less likely to be an issue.
Will a coronavirus vaccine need to be given annually?
When a vaccine is licensed, we will only have information about length of immunity for as long as we are from the trials. For example, if the first people in the study were vaccinated in July 2020 and the vaccine is licensed in December 2020, we will only have information about the immune response up to 5 months after vaccination. The vaccine manufacturer will likely continue to monitor vaccine recipients for several months or more, so that over time, we will continue to get a better picture of the durability of immunity. With this information, we will be better able to understand whether vaccines against COVID-19 will require annual dosing like influenza.
Is a coronavirus vaccine necessary?
SARS-CoV-2 infections can be a minor hindrance or lead to severe disease or even death. While hygiene measures such as social distancing, handwashing, and wearing masks offer some help, the best way to stop this virus is to generate SARS-CoV-2-specific immunity. This specific immunity can be achieved in one of two ways — through illness or vaccination. Since illness could lead to severe disease or death, vaccination is a better alternative as long as safe and effective vaccines can be developed.
How long before a coronavirus vaccine takes effect?
Generally speaking, it takes a week or two for immunity to develop following vaccination, but the specific timeline for any coronavirus vaccine will depend to some extent on which type of vaccine is licensed. For example, a live, weakened vaccine requires time to reproduce in the body, whereas an inactivated vaccine is given at a dose that will generate immunity. On the other hand, because the live, weakened vaccine reproduces to generate immunity, it might provide a more robust immune response than an inactivated vaccine
Univ. of Oxford Vaccine: Ready by September?!
Meet Sarah Gilbert!
By Shlomo Maital

Prof. Sarah C. Gilbert, Univ. of Oxford
A Bloomberg News report has optimistic information about the University of Oxford’s burgeoning COVID-19 vaccine, which, Bloomberg says, could be ready by September.* In a deal with Astra-Zeneca, the latter says it could quickly prepare as many as 2 billion doses. And sell them on a not-for-profit basis! And there is a lovely human side to this medical tale. So – meet Sarah Gilbert. She might just save your life.
“In April, Sarah Gilbert’s three children, 21-year-old triplets all studying biochemistry, decided to take part in a trial for an experimental vaccine against Covid-19. It was their mother’s vaccine—she leads the University of Oxford team that developed it—but there wasn’t a big family talk. “We didn’t really discuss it as I wasn’t home much at the time,” Gilbert told me recently. She’d been working around the clock, as one does while trying to end a pandemic, and at any rate wasn’t worried for her kids. “We know the adverse event profile and we know the dose to use, because we’ve done this so many times before,” she says. “Obviously we’re doing safety testing, but we’re not concerned.” With safety low on her list of worries (her triplets are fine), Gilbert is focused on quickly determining how effective the vaccine will be and how it will be made. In April, Oxford struck a deal with British pharmaceutical giant AstraZeneca Plc to spearhead global manufacturing and distribution and help run more trials around the world. AstraZeneca has agreed to sell the vaccine on a not-for-profit basis during the crisis if it proves effective and has lined up deals with multiple manufacturers to produce more than 2 billion doses.
Prof. Gilbert shuns the limelight. But she may soon well be one of the most famous scientists in the world:
” Gilbert has been all over the British press, but she appears to regard public attention as a distraction. For more than two decades she worked anonymously, developing vaccines while also, of necessity, churning out endless grant applications. Her research was rarely discussed outside scientific circles. Now she’s leading one of the most high-profile and advanced vaccine candidates against Covid-19, with Phase III, or final-stage, trials under way involving thousands of people in Brazil, South Africa, the U.K., and, soon, the U.S. Money is no longer a struggle. At the end of April, crunching a process that normally takes about five years into less than four months, Gilbert and her colleagues at Oxford’s Jenner Institute started a human trial on 1,100 people. When Gilbert testified before a parliamentary committee in early July, one member compared her effort to going into a shed and coming out with a jet engine. Gilbert’s team has leapfrogged other vaccine contenders to the point where it will likely finish vaccinating subjects in its big 10,000-person efficacy trial before other candidates even start testing on that scale, Kate Bingham, chair of the U.K. government’s Vaccine Taskforce, told the parliamentary committee in early July. “She’s well ahead of the world,” Bingham said. “It’s the most advanced vaccine anywhere.”
This is no overnight success. Gilbert has labored for years in her laboratory, to develop the knowledge and skill that perhaps has prepared her for this moment, to save the world:
” Gilbert, who is 58, has the hyper-efficient, serious demeanor you’d expect from someone who might be on the cusp of a breakthrough and hasn’t a minute to spare. When I first called her in early March, she abruptly ended the conversation after 10 minutes to speak to someone about the technical process of manufacturing the vaccine. It would have been crazy to take offense. Gilbert says she wakes up at around 4 a.m. most days “with lots of questions in my head,” works from home for a few hours, then rides her bicycle to the institute, where she works into the evening. The Oxford team, just a handful of people in January, now comprises roughly 250. The vaccine is a so-called viral vector type based on years of research by Gilbert and Adrian Hill, the head of the Jenner Institute. Traditional vaccines are made with a weakened or inactivated form of the germ that causes infection to stimulate an immune response. Those vaccines aren’t easy to develop and produce quickly. The Oxford team has developed a technology that can speed up the process by using a harmless virus as a kind of Trojan horse to carry the genetic material of a pathogen into cells to generate an immune response. In the case of Covid-19, Gilbert has taken a chimpanzee adenovirus (a common cold virus) and inserted genetic material from the surface spike protein of the SARS-CoV-2 virus as a way of tricking the immune system to fight back. The chimp adenovirus platform stimulates both antibodies and high levels of killer T-cells, a type of white blood cell that helps the immune system destroy infection.
The Oxford – Gilbert vaccine could still fail. But I don’t think so. Gilbert is confident.
“Gilbert has voiced remarkable confidence in her chances, saying the Oxford vaccine has an 80% probability of being effective in stopping people who are exposed to the novel coronavirus from developing Covid-19. She has said she could know by September. Asked by MPs in early July whether the world would have to struggle through the winter without a vaccine, Gilbert said, “I hope we can improve on those timelines and come to your rescue.” “We could say, ‘OK, we can start tomorrow.’ We don’t have to make 10 different varieties of this. We knew it could be manufactured”
One American in Three Will Refuse a COVID-19 Vaccine
By Shlomo Maital
I’m not sure you will believe this. I could barely believe it.
A CNN public opinion poll in the United States revealed:
,,, we’re getting a closer look at how some Americans feel about the pandemic. A new national poll surveyed 1,000 adults and found 35% of Americans say they won’t get the coronavirus vaccine. Twenty-nine percent of Americans say they will definitely get the vaccine. Another third said probably.
No need for further comment. One American in three will turn down a COVID-19 vaccine when it is offered to them. And another third said, well, probably, not certain.
Two-thirds of Americans are not 100% certain they will seek a vaccine, when it is available.
A large part of the world is deeply worried, that they will not be able to get the vaccine, because the rich countries, pursuing America First policies, will keep it for themselves.
And in America (first), two-thirds are not 100% sure they will accept the vaccine.
So, many people will die through ignorance and conspiracy theories fed by social media.
We have seen in the past outbreaks of measles, in the US and elsewhere, through abysmal ignorance.
Here we go again.
What in the world has happened to this once-great nation?
p.s. President Donald Trump is busy promoting Goya beans and other products from the Oval Office. I did not make that up.
The Moderna mRNA Vaccine, Phase 1
5 Things We Need to Know – and Why We Should Celebrate (a Bit)
By Shlomo Maital

A sign of the times: A jargon-filled academic article published in the New England Journal of Medicine,* about a very small Phase 1 trial of a COVID-19 vaccine, has stock markets rising, or even soaring, social media buzzing, …. But — what is this really about? What is the state of Moderna’s vaccine, in simple language, as Moderna gears up for massive Phase 3 trials?
Here are 5 things you need to know and understand. From what I understand, the Moderna vaccine IS a big deal. It offers us great hope. Let’s try to understand why. This blog is long – nearly 1,500 words.
First – what’s the story about Moderna?
Moderna is a US biotech company based exclusively on messenger RNA (mRNA) (see below), in Cambridge, Massachusetts. (RNA is ribonucleic acid.)
Messenger RNA is RNA that tells the ‘ribosome’ (the protein factory inside the cell) which proteins to make and how to make them, by assembling amino acids.
The Moderna technology inserts synthetic (manmade) mRNA into living cells in order to reprogram the cells to develop immune responses. It is a novel technique abandoned by several large pharmaceutical and biotechnology companies who all failed to overcome the side effects of inserting RNA into cells. As of May 2020, no mRNA drug had been approved for human use. Moderna’s decision to try to develop a COVID-19 vaccine based on this risky unproven technology was a huge leap of faith. And, it may have worked.
Previously, Moderna conducted mostly failed trials with AstraZeneca, and in orphan diseases with Alexion Pharmaceuticals. In 2014, Moderna moved to focus on lower-margin mRNA vaccines. The strategic change led industry experts, and even Moderna employees, to question whether the company would survive. It looked bleak.
In December 2018, Moderna became the biggest initial biotech public offering of shares (IPO) in history, raising US$600 million for 8% of its shares, implying that the company was worth $7.5 billion – this, despite cumulative losses of $1.5 billion and equity raised of $3.2 billion.
As of May 2020, Moderna was valued at $30 billion, but none of its mRNA molecules had reached large clinical trials, and several had failed due to side-effects. It looked like a bubble to many.
And then came the huge leap into the unknown – the race to create a COVID-19 virus.
In July 2020, Moderna announced that its mRNA COVID-19 vaccine candidate in Phase 1 clinical testing had led to production of neutralizing antibodies in healthy adults. * And – the side effects were not serious (headaches, nausea). The article was peer-reviewed in the leading medical journal, New England Journal of Medicine.
Now, here are a few more things we need to know, from a trusted website.**
** https://horizon-magazine.eu/article/five-things-you-need-know-about-mrna-vaccines.html
1. “Vaccines based on messenger RNA are a whole new type of vaccine If an mRNA vaccine was approved for coronavirus, it would be the first of its type. ‘It’s a very unique way of making a vaccine and, so far, no (such) vaccine has been licenced for infectious disease,’ said Prof. Isabelle Bekeredjian-Ding, Paul Ehrlich Institute, Germany
“Vaccines work by training the body to recognize and respond to the proteins produced by disease-causing organisms, such as a virus or bacteria. Traditional vaccines are made up of small or inactivated doses of the whole disease-causing organism, or the proteins that it produces, which are introduced into the body to provoke the immune system into mounting a response.
“But mRNA vaccines, in contrast, trick the body into producing some of the viral proteins itself. They work by using mRNA, or messenger RNA, which is the molecule that essentially puts DNA instructions into action. Inside a cell, mRNA is used as a template to build a protein. ‘An mRNA is basically like a pre-form of a protein and its (sequence encodes) what the protein is basically made of later on,’ said Prof. Bekeredjian-Ding.
“To produce an mRNA vaccine, scientists produce a synthetic version of the mRNA that a virus uses to build its infectious proteins. This mRNA is delivered into the human body, whose cells read it as instructions to build that viral protein, and therefore create some of the virus’s molecules themselves. These proteins are solitary, so they do not assemble to form a virus. The immune system then detects these viral proteins and starts to produce a defensive response to them.
This is crucial. Vaccines are traditionally made by weakening or killing the virus or bug that causes illness. If they are not made properly, they can make people ill. So manufacturing them is very difficult, costly and time-consuming. mRNA vaccines are not dangerous, because the RNA they introduce triggers an immune reaction, but it cannot cause the illness itself!
- The mRNA vaccines could be more potent and straightforward to produce than traditional vaccines
“There are two parts to our immune system: innate (the defences we’re born with) and acquired (which we develop as we come into contact with pathogens). Classical vaccine molecules usually only work with the acquired immune system and the innate immune system is activated by another ingredient, called an adjuvant. Interestingly, mRNA in vaccines could also trigger the innate immune system, providing an extra layer of defence without the need to add adjuvants.
‘All kinds of innate immune cells are being activated by the mRNA,’ said Prof. Bekeredjian-Ding. ‘This primes the immune system to get prepared for an endangering pathogen and thus the type of immune response that is triggered is very strong.’
“There is still a lot of work to be done to understand this response, the length of the protection it could give and whether there are any downsides. Prof. Bekeredjian-Ding also explains that because you’re not introducing the whole virus into the body, the virus can’t mount its own self-defence and so the immune system can concentrate on creating a response to the viral proteins without interference by the virus. And by getting the human body to produce the viral proteins itself, mRNA vaccines cut out some of the manufacturing process and should be easier and quicker to produce than traditional vaccines. ‘In this situation, the major benefit is that it’s easy to produce (and) it will also probably be relatively easy to do an upscaling of production, which of course, is very important if you think about deployment throughout Europe and the world,’ said Prof. Bekeredjian-Ding. ‘It’s a very unique way of making a vaccine and, so far, no (such) vaccine has been licenced for infectious disease.’
- There are a lot of unknowns. “Because mRNA vaccines are only now beginning to be tested in humans, there are a lot of fairly basic unknowns which can only be answered through human trials. ‘What is really the current challenge, I think, is to understand whether these vaccines will really be able to mount a sufficiently protective immune response in the human and to understand, for example, which quantities of mRNA will be needed to do this,’ said Prof. Bekeredjian-Ding.
“Other outstanding questions include whether the proteins that have been chosen for the vaccine are the right ones to prevent a coronavirus infection in the body, how targeted the immune response is to this particular coronavirus, how long any immunity would last, and whether it causes side-effects such as increased inflammatory responses like redness and swelling or, in the worst case, aggravates disease.”
- It would be possible to vaccinate on a large scale. (NOTE: THIS IS A BIGGIE!)
“Once an mRNA vaccine has been approved, which could take 12-18 months, it should be easy to scale up production. Because the manufacturing process is shorter than for other vaccines – Prof. Bekeredjian-Ding estimates a few months rather than 1-2 years for conventional vaccines – there is potential for these vaccines to be scaled up quickly. This is useful in the context of coronavirus, which will likely need mass immunization programs.
‘I think we will need a very high population coverage, but it depends a little bit on the countries and the epidemiology,’ said Prof. Bekeredjian-Ding. ‘In the countries where coronavirus has been spreading very fast, we also expect that there’s many people who have been in contact with the virus and who have actually mounted a natural immune response. But on the other hand, if you look at Germany, for example, right now we’re all at home, barred, and not allowed to leave the house except for necessities.
And…I can’t resist adding this. The Chief Medical Officer of Moderna is Dr. Tal Zaks. He is Israeli. He studied at Ben Gurion University of the Negev. Regarding Moderna’s vaccine, he said that its experimental anti-COVID-19 vaccine “actually works,” after tests on a small number of volunteers, and that it will start Phase 3 testing on thousands of people in July.
“We got the first results today… and today we are showing that it actually works… we are able to stimulate the immune system,” Dr. Zaks said.
Dr. Zaks believed in Moderna’s mRNA vaccine from the outset, when many did not. Can we hope that this vaccine will end up saving many many lives, all over the world?
* An mRNA Vaccine against SARS-CoV-2 — Preliminary Report New England Journal of Medicine. July 15, 2020.
Can an Old Soviet-Era Idea Help Fight this New Virus?
By Shlomo Maital

Dr. Marina Voroshilova and Dr. Mikhail Chumakov, left
Sometimes, you battle a new foe, like the novel coronavirus, with an old idea – even one dating from Soviet Russia. Writing in today’s New York Times, Andrew Kramer describes a 60-year-old idea used by two virologists in the USSR, Marina Voroshilova and Mikhail Chumakov, that may be helpful in today’s pandemic.
It sounds preposterous – use, say, polio vaccine to fight COVID-19? Really?
Here is the basic idea:
“We formed a kind of line,” Dr. Peter Chumakov, who was 7 at the time, recalled in an interview. Into each waiting mouth, a parent popped a sugar cube laced with weakened poliovirus — an early vaccine against a dreaded disease. “I was eating it from the hands of my mother.” Today, that same vaccine is gaining renewed attention from researchers — including those brothers, who all grew up to be virologists — as a possible weapon against the new coronavirus, based in part on research done by their mother, Dr. Marina Voroshilova.
“Dr. Voroshilova established that the live polio vaccine had an unexpected benefit that, it turns out, could be relevant to the current pandemic: People who got the vaccine did not become sick with other viral illnesses for a month or so afterward. She took to giving the boys polio vaccine each fall, as protection against flu. Now, some scientists in several countries are taking a keen interest in the idea of repurposing existing vaccines, like the one with live poliovirus and another for tuberculosis, to see if they can provide at least temporary resistance to the coronavirus. Russians are among them, drawing on a long history of vaccine research — and of researchers, unconcerned about being scoffed at as mad scientists, experimenting on themselves.
“Experts advise that the idea — like many other proposed ways of attacking the pandemic — must be approached with great caution. “We are much better off with a vaccine that induces specific immunity,” Dr. Paul A. Offit, a co-inventor of a vaccine against the rotavirus and professor at the Perelman School of Medicine at the University of Pennsylvania, said in a telephone interview. Any benefits from a repurposed vaccine, he said, are “much shorter lived and incomplete,” compared with a tailored vaccine. Still, Dr. Robert Gallo, a leading advocate of testing the polio vaccine against coronavirus, said that repurposing vaccines is “one of the hottest areas of immunology.” Dr. Gallo, director of the Institute of Human Virology at the University of Maryland School of Medicine, said that even if the weakened poliovirus confers immunity for only a month or so, “it gets you over the hump, and it would save a lot of lives.”
The current pandemic has brought a tidal wave of creative ideas. Most fail. A few succeed. Even preposterous ideas, like enlisting polio vaccine, are worth a shot. The novel coronavirus is wily, clever, sneaky and in some places mutating; so we humans need to be at least half as smart as it is.
Don’t Count Too Much on a Vaccine
By Shlomo Maital

Dr. William Haseltine
The Tyee is an independent online Canadian news magazine that primarily covers British Columbia. [Thetyee.ca]. Contributing writer Andrew Nikiforuk writes about a world-leading virologist Dr. William Haseltine, vilified in the past for doubting an AIDS vaccine could be produced (apparently, it can’t), and now sharing doubts about a COVID-19 vaccine. His views are worth heeding…. Warning: This blog is 1,000 words, twice as long as usual!
“William Haseltine: People should regard everyone they meet as infected and act accordingly. ‘That’s the only safe assumption you can make. And don’t assume that if you’ve been infected, you’re protected.’
When William Haseltine told a group of fellow scientists in 1986 that an AIDS vaccine would be unlikely because of the difficult nature of the virus, he was booed off the stage. His colleagues even threw stuff at him. “But we still don’t have a vaccine for AIDS,” he recently told Reuters. “We don’t know for sure that a [COVID-19] vaccine won’t be developed, but I can say with the same conviction — don’t count on it.”
In the last couple of weeks the virologist also has offered some jarring observations on the nature of the coronavirus, self-promotion by drug labs, the hazards of rapid reopenings and our global unpreparedness for what is yet to come.
Here are Haseltine’s eight key observations…
- Beware of those who purvey premature hope.
Haseltine’s years of experience cause him to caution against being manipulated by emotion. A number of firms have been giving “a false impression of progress” on the vaccine front, he worries. Cambridge-based Moderna, for example, made headlines last week with news of a safety trial on just eight healthy individuals for its vaccine. The value of the company’s stock exploded. Although the company said their experimental vaccine raised neutralizing antibodies, it said nothing about levels
- Even a vaccine that works likely won’t solve the pandemic.
Haseltine also wants citizens to appreciate this bit of wisdom: a vaccine will not likely end this pandemic for several reasons.
For starters the most affected population, people over the age of 60, are the most difficult population to develop vaccines for. As the immune system ages, the effectiveness and duration of vaccines wanes with it. “It is very difficult to develop a vaccine for older people,” notes Haseltine.
Second, coronaviruses make difficult vaccine candidates because they produce many proteins that allow them to trick and evade the immune system.
Third, Haseltine doesn’t think an adenovirus-based vaccine such as the one proposed by CanSino Biologics, and now being tested in Halifax, will do the trick either.
- A flattened curve is not a road to victory.
Haseltine also thinks many people aren’t taking the disease seriously enough. The veteran virus fighter compares COVID-19 to polio. It, too, was a cold virus with a nasty bite. One in 200 people infected came down with paralysis and of those 10 to 15 percent died of muscle paralysis. It, too, spread through what white coats call “the oral-fecal route” on people’s hands and contaminated surfaces.
As the world experiments with reopening after the first wave, often without adequate testing, contract tracing and isolation facilities in place, people should regard everyone they meet as infected and act accordingly.
“That’s the only safe assumption you can make,” he said. “And don’t assume that if you’ve been infected, you’re protected.” He advises people not to let down their guard or stop wearing a mask in crowded places until their city and region hasn’t recorded a COVID-19 case for a month.
- ‘Herd immunity’ is a dubious prospect.
Haseltine also thinks you can forget about herd immunity as some kind of saving grace. There is a reason that we all get colds every year and that’s because immunity to the four corona viruses that cause colds doesn’t last long.
“There’s no such thing as herd immunity for this disease. I doubt it will ever exist,” Haseltine said in a Reuters interview, because “people who have had it are getting reinfected.” He thinks Sweden made a bad mistake going for herd immunity, and then cites the nation’s death rate which is higher than any other Scandinavian country.
- We remain woefully unprepared.
The next thing Haseltine wants you to think about is our chronic and ongoing lack of pandemic preparedness. COVID-19 caught the world with its pants down because governments and corporations ignored all the warnings. If you want to know how predictable pandemics can be just watch the film Contagion, says Haseltine.
Nearly 15 years ago the emergence of SARS and then MERS demonstrated that coronaviruses could be an existential threat. Although researchers started work on 20 potential drugs for these coronaviruses, they all got shelved.
“Those drugs lay dusty on the shelves in China, in Singapore, in Hong Kong, in Europe, in the United States, and in the [United Arab] Emirates and Saudi [Arabia] where they were discovered and shown to work in animal models of both SARS and MERS.” The reason: there was no economic model to develop them. Haseltine thinks it is more likely researchers will find a suitable drug treatment for the virus before they develop a safe vaccine.
- Nature is not nearly as controllable as we wish.
The pandemic is also sending people a deep and profound message, says Haseltine. “We are part of Nature. We don’t control Nature. Do we control volcanoes? Do we control hurricanes? Viruses are part of nature and their job is to grow in us,” Haseltine recently told Reuters.
- Much bigger threats loom.
Globalization and human population growth have created pretty good ecosystems for new colonizing viruses. Every day the viral world makes trillions of random mutations and some of these mutations produce viruses that can adapt to human environments better than others. More pandemonium is coming, warns Haseltine.
“It is only a matter of time before a coronavirus that is far more lethal and contagious than this one emerges to ravage the world’s population,” says Haseltine. “When that happens, we will no longer be talking about a global death toll in the ‘mere’ hundreds of thousands.” He also suspects the world is overdue for a deadly influenza outbreak capable of removing one to two billion people from the planet.
- Changes in behavior can save us now. And far more certainly than any vaccine.
Last but not least, we should pay more attention to the most important part of this story: changing human behaviour can stop COVID-19 dead in its tracks.
Why Mab is Fab: A Monoclonal Antibody Defeats COVID-19
By Shlomo Maital
Scientists all over the world are desperately searching for a ‘silver bullet’ – a magical compound that can defeat the insidious, devious and evil novel coronavirus. It may be that scientists at Israel’s Institute for Biological Research have found it.
First, a small science lecture.
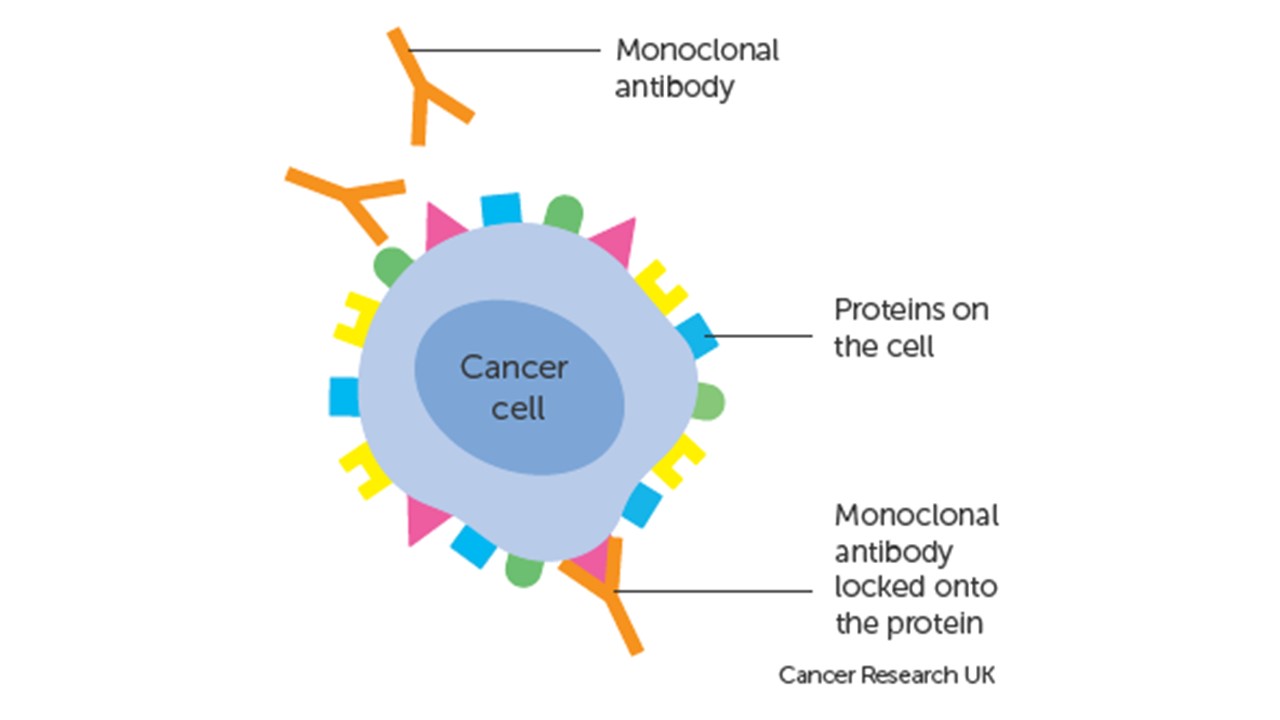
Antibodies are large, Y-shaped proteins produced mainly by plasma cells in the body, that are used by the body’s immune system to neutralize pathogenic bacteria and viruses that make us ill or kill us.
Monoclonal antibodies (Mab’s, for short, the suffix added to drugs produced in this way) are antibodies made by identical immune cells that are all clones of a unique parent cell. Monoclonal antibodies bind to the same part of an antigen [the bad stuff from a virus] that is recognized by the antibody.
Put it this way: Monoclonal antibodies (Mab’s) are like little guided missiles, fired by the body at, for example, the spikes on the coronavirus that poke through cell walls and infect it. [See the diagram above]. Those little guided missiles neutralize those spikes and prevent the virus from infecting human cells by poking through their walls. The body then destroys the virus before it does damage.
These Mab’s have been used so far mainly as promising anti-cancer drugs, as part of so-called immunotherapy. The anti-cancer drugs zero in on cancer cells and kill them. The key is the word “monoclonal” – unique little antibodies that aim specifically, uniquely, at an offending invading virus or cancer cell.
A press announcement stated: “The Israel Institute for Biological Research (IIBR) has completed a groundbreaking scientific development, determining an antibody that neutralizes the coronavirus, SARS-CoV-2, according to a statement by the Defense Ministry. [That is the scientific name for the virus that causes COVID-19]. This scientific breakthrough has three key parameters: The antibody is monoclonal, new and refined, and contains an exceptionally low proportion of harmful proteins; the institute has demonstrated the ability of the antibody to neutralize the coronavirus; the antibody was specifically tested on the aggressive coronavirus. Based on comprehensive scientific publications from around the globe, it appears that the IIBR is the first institution to achieve a scientific breakthrough that meets all three of the aforementioned parameters simultaneously,” the Defense Ministry said in a statement on behalf of the institute.
The breakthrough is now being patented.
In addition, to produce the COVIDi-19 Mab, “IIBR and the small southern town of Yeruham, Israel, on Monday night announced they have big plans to open Israel’s first vaccine production facility, in partnership with one of two prospective international pharmaceutical companies.”
All over the world, vaccine production facilities are ramping up, long before the vaccines themselves have been proven safe and effective. So once a vaccine is found, it can be produced in large amounts quickly.
The Mab approach is promising, because it is a compound that can be taken orally, rather than by injection.
Let us hope that this report is accurate and that the anti-corona Mab really works and can be produced massively and quickly, and safely. Let’s hope the Israeli Mab is indeed fab.
Understanding Vaccine Science: A Primer
By Shlomo Maital

Here is my effort to understand where we stand, with regard to a COVID-19 vaccine.
There are several different types of vaccines, each with its own strategy.
- Live attenuated vaccines. These use the virus itself, weaken it, and inject it; the body’s immune system is alerted and springs into action, developing antibodies that can defeat the virus if and when it invades the human body. This is how vaccines against measles and mumps work. Measles vaccine has existed since 1950 and still is effective; measles has not mutated to defeat it.
- Inactivated vaccines. These use ‘dead’ viruses. Even though ‘dead’ the presence of the virus in the body activates the immune system. Vaccines based on this approach are effective against hepatitis and polio. Polio vaccine has been effective since the early 1950’s.
- Subunit vaccines. These vaccines use specific pieces of the virus, key pieces, to activate immunity and neutralize the virus if and when it invades the human body. Examples: vaccines against whooping cough and shingles.
- Toxoid vaccines. These use toxins produced by the germs, to trigger the immunity of the body that attacks the harmful toxins. E.g. vaccines against diphtheria and tetatnus.
- DNA/ RNA vaccines. These are the newest types of vaccine.
At Emory University, in Atlanta Georgia, for example, a new type of mRNA vaccine against COVID-19 is now being tested in humans (an Emory medical student). Here is how it works: “messenger RNA” is the protein made by the virus, found on those spikes you see in cartoon illustrations, these spikes poke through the cell walls to invade the cell and use its DNA to reproduce. mRNA vaccines teach the body to produce, identify and attack those key proteins, neutralize them and hence prevent the virus from poking through cell walls.
All over the world, desperate races are underway to develop a COVID-19 vaccine. All these different approaches are being used. Many labs are trying to use existing vaccines against related illnesses and adapt them.
A major problem: There has not yet been a vaccine effective against coronavirus (e.g. the common cold, which is a variant of corona). And the DNA/RNA approach is relatively new and untried.
With so many bright hard-working scientists at work day and night, there will be a breakthrough. And I believe it will come sooner rather than later. One of the key sparkplugs of creativity is desperation, and the world today is desperate for a vaccine. Add to that the profit motive – many billions of doses will be needed.
The Race to a COVID-19 Vaccine: Q&A
By Shlomo Maital

Where do we stand in the quest for a safe effective COVID-19 vaccine?
More than 2.2 million persons worldwide have contracted the virus and of those, 154,783 have died. That is a 6.8% death rate. But wait – there are far far more cases worldwide than those we know about. Deaths are certain; cases are a guess. If we use a 1% to 1.5% death rate, we can guess that between 10 million and 15 million persons worldwide have contracted the illness. Only an effective vaccine will put a clear end to this crisis, in which COVID-19 is already the #1 cause of death in the US.
This Q&A is based on an informative survey published in a reputable website, livescience.com, by staff writer By Nicoletta Lanese, two days ago: (Warning: this blog is long, 1895 words…sorry).
* https://www.livescience.com/coronavirus-covid-19-vaccine-timeline.html
When will a vaccine be ready?
“Here’s why it probably can’t be developed any sooner than 12 to 18 months.
“More than 60 candidate vaccines are now in development, worldwide, and several have entered early clinical trials in human volunteers, according to the Some groups aim to provoke an immune response in vaccinated people by introducing a weakened or dead SARS-CoV-2 virus, or pieces of the virus, into their bodies. The vaccines for measles, influenza, hepatitis B and the vaccinia virus, which causes smallpox, use these approaches, according to the U.S. Department of Health & Human Services. Although tried-and-tested, using this approach to develop these conventional vaccines was labor-intensive, requiring scientists to isolate, culture and modify live viruses in the lab.
That initial process of just creating a vaccine can take 3 to 6 months, “if you have a good animal model to test your product,” Raul Andino-Pavlovsky, a professor in the Department of Microbiology and Immunology at the University of California, San Francisco, told Live Science. “
Are there short cuts? How fast is the US working on a vaccine?
“The first COVID-19 vaccine to enter clinical trials in the United States, for example, uses a genetic molecule called mRNA as its base. Scientists generate the mRNA in the lab and, rather than directly injecting SARS-CoV-2 into patients, instead introduce this mRNA. By design, the vaccine should prompt human cells to build proteins found on the virus’ surface and thus trigger a protective immune response against the coronavirus. Other groups aim to use related genetic material, including RNA and DNA, to build similar vaccines that would interfere with an earlier step in the protein construction process. But there’s one big hurdle for mRNA vaccines. We can’t be sure they will work. As of yet, no vaccine built from a germs’ genetic material has ever earned approval, Bert Jacobs, a professor of virology at Arizona State University and member of the ASU Biodesign Institute’s Center for Immunotherapy, Vaccines and Virotherapy, told Live Science. Despite the technology having existed for almost 30 years, RNA and DNA vaccines have not yet matched the protective power of existing vaccines, National Geographic reported.
In this high-stakes competition, is there also collaboration?
“Assuming these unconventional COVID-19 vaccines pass initial safety tests, “will there be efficacy?” Jacobs said. “The animal models suggest it, but we’ll have to wait and see.” “Because of the emergency here, people are going to try many different solutions in parallel,” Andino-Pavlovsky said. The key to trialing many vaccine candidates at once will be to share data openly between research groups, in order to identify promising products as soon as possible, he said.
Could a COVID-19 vaccine be potentially dangerous and do damage?
For sure.
“Designing a vaccine that grants immunity and causes minimal side effects is no simple task. A coronavirus vaccine, in particular, poses its own unique challenges. Although scientists did create candidate vaccines for the coronaviruses SARS-CoV and MERS-CoV, these did not exit clinical trials or enter public use, partly because of lack of resources, Live Science previously reported. “One of the things you have to be careful of when you’re dealing with a coronavirus is the possibility of enhancement,” Fauci said in an interview with the journal JAMA on April 8. Some vaccines cause a dangerous phenomenon known as antibody dependent enhancement (AED), which paradoxically leaves the body more vulnerable to severe illness after inoculation. Candidate vaccines for dengue virus, for example, have generated low levels of antibodies that guide the virus to vulnerable cells, rather than destroying the pathogen on sight, Stat News reported. Coronavirus vaccines for animal diseases and the human illness SARS triggered similar effects in animals, so there’s some concern that a candidate vaccine for SARS-CoV-2 might do the same, according to an opinion piece published March 16 in the journal Nature. Scientists should watch for signs of AED in all upcoming COVID-19 vaccine trials, Fauci said. Determining whether enhancement is occurring could happen during initial animal studies, but “it is still unclear how we will look for AED,” Jacobs said.
Are there specific dangers in developing a COVID-19 vaccine?
A successful coronavirus vaccine will snuff the spread of SARS-CoV-2 by reducing the number of new people infected, Andino-Pavlovsky said. COVID-19 infections typically take hold in so-called mucosal tissues that line the upper respiratory tract, and to effectively prevent viral spread, “you need to have immunity at the site of infection, in the nose, in the upper respiratory tract,” he said. These initial hotspots of infection are easily permeated by infectious pathogens. A specialized fleet of immune cells, separate from those that patrol tissues throughout the body, are responsible for protecting these vulnerable tissues. The immune cells that protect mucosal tissue are generated by cells called lymphocytes that remain nearby, according to the textbook “Immunobiology: The Immune System in Health and Disease” (Garland Science, 2001).
“It’s like your local police department,” Andino-Pavlovsky told Live Science. But not all vaccines prompt a strong response from the mucosal immune system, he said. The seasonal influenza vaccine, for example, does not reliably trigger a mucosal immune response in all patients, which partly explains why some people still catch the respiratory disease after being vaccinated, he said.
“Even if a COVID-19 vaccine can jumpstart the necessary immune response, researchers aren’t sure how long that immunity might last, Jacobs added. While research suggests that the coronavirus doesn’t mutate quickly, “we have seasonal coronaviruses that come, year in [and] year out, and they don’t change much year to year,” he said. Despite hardly changing form, the four coronaviruses that cause the common cold keep infecting people — so why haven’t we built up immunity?
Could the COVID-19 virus pose special problems?
“Perhaps, there’s something odd about the virus itself, specifically in its antigens, viral proteins that can be recognized by the immune system, and that causes immunity to wear off. Alternatively, coronaviruses may somehow fiddle with the immune system itself, and that could explain the drop-off in immunity over time, Andino-Pavlovsky said. To ensure a vaccine can grant long-term immunity against SARS-CoV-2, scientists will have to address these questions. In the short term, they’ll have to design experiments to challenge the immune system after vaccination and test its resilience through time, Jacobs said. In a mouse model, such studies could take “at least a couple of months,” he said. Scientists cannot conduct an equivalent experiment in humans, but can instead compare natural infection rates in vaccinated people to those of unvaccinated people in a long-term study. “When you have the luxury, you look at this for five years, 10 years to see what happens,” Andino-Pavlovsky added.
How will they ensure that a COVID-19 vaccine is safe?
“Unlike an antiviral treatment for COVID-19 that can be given to patients already infected with the virus, a vaccine must be tested in diverse populations of healthy people. “Because you give it to healthy people, there’s an enormous pressure to make sure it’s absolutely safe,” Andino-Pavlovsky said. What’s more, the vaccine must work well for people of many ages, including the elderly, whose weakened immune systems place them at heightened risk of serious COVID-19 infection. “Initially, safety studies will be done in small numbers of people,” likely fewer than 100, Jacobs said. A vaccine may be approved based on these small studies, which can take place over a few months, and then continually monitored as larger populations become vaccinated, he added. “That’s just my guess.”
[Note: The high and growing death toll from COVID-19 may justify some speed-up and short-cuts].
So what are the various stages that a vaccine must undergo, before it can be mass produced?
“Any potential vaccine will need to pass a safety trial, known as a Phase 1 trial, which also helps determine the needed dose. The next step is a larger trial in 100 to 300 people, called a Phase 2, which looks for some biological activity, but can’t say for sure if the drug is effective. If a vaccine candidate prompts a promising immune response in Phase 2 clinical trials, after passing safety tests in Phase 1, it’s possible that the FDA could approve such a vaccine for emergency use “before the 18-month period that I said,” Fauci said in the JAMA interview. “If you get neutralizing antibodies,” which latch onto specific structures on the virus and neutralize it, “I think you can keep moving forward on it,” Jacobs said. Normally, a vaccine would then enter Phase 3 clinical trials, which include hundreds to thousands of people.
“So adding up these steps, each of which will likely take 3 to 6 months, it’s very unlikely we would be able to find a vaccine that is safe and effective in less than 12 months — even if many of these steps could be done in parallel.
Can it be mass-produced? How?
“Then comes the issue of manufacturing billions and billions of doses of a new vaccine whose ingredients we don’t yet know. Bill Gates has said that the Gates Foundation will fund the construction of factories for seven coronavirus vaccine candidates, equipping the sites to produce a wide variety of vaccine types, Business Insider reported.
[Neanderthal Conservative groups have attacked Gates, making false and inflammatory claims about him].
“Even though we’ll end up picking at most two of them, we’re going to fund factories for all seven, just so that we don’t waste time in serially saying, ‘OK, which vaccine works?’ and then building the factory,” Gates said. Even if a fairly promising vaccine surfaces by 2021, and can be mass-produced, the search won’t end there. “Especially with trying to get something out this quickly, we may not get the best vaccine out there right away,” Jacobs said. Ideally, an initial vaccine will grant immunity for at least one to two years, but should that immunity wane, a longer lasting vaccine may have to be deployed. Historically, so-called live attenuated vaccines that contain a weakened virus tend to perform most reliably over extended periods of time, Andino-Pavlovsky said.
“That may be what we need in the long run,” he said. And research into coronavirus immunity should continue, regardless, “not only for COVID-19, but for the next coronavirus that comes.

