
You are currently browsing the category archive for the ‘Uncategorized’ category.
by Shlomo Maital
Today’s Jerusalem Post reports on a fascinating Israel-India collaboration, to develop something the world has needed for a very long time, since the start of the pandemic: a quick (instant) test!
One of the key implications of a 30-second test is that air travellers will be able to confirm they are virus-free instantly — and board without hassle. This could save civil aviation, which is in a desperate crisis — in the US alone, some 130,000 civil aviation employees face permanent layoffs.
Here is the report by Maayan Jaffee-Hoffman:
“A 30-second coronavirus detection test being developed by India and Israel should be ready in “a matter of days,” Israeli Ambassador to India Ron Malka told the Indian news agency PTI on Friday. “All the thresholds have been passed.”
The operation has been dubbed “Open Skies,” and Malka said he believes the testing kit will enable the world to begin opening the skies, since the technology simply requires a person to blow into a tube and the results become available in less than a minute. It is also very cheap to carry out, as the results are delivered locally without the logistics and cost of sending the sample to a lab. ”
by Shlomo Maital
Policy begins with measurement. If you measure wrongly, you act wrongly. Result: Fiasco.
My country Israel is deep in a COVID-19 second wave, far worse than the first, with 7,000 and more new cases daily, for a small country of some 9 million people. There are nearly 900 people in intensive care – stretching ICU capacity to the limit. Medical staff, working non-stop since February, are crushed under the burden. And now, a country-wide severe lockdown, closing businesses and schools, closing everything.
So why is this a fiasco? It is explained clearly in this article: “This Overlooked Variable Is the Key to the Pandemic. It’s not R0.” ZEYNEP TUFEKCI. SEPTEMBER 30, 2020 The Atlantic.
This is a very long blog. So here is a brief summary. Political leaders, guided by public health experts, are focused on R0 – this is the AVERAGE number of people infected by one person already infected. R0 bigger than one: exponential spread. R0 less than one: negative exponential decline. So the goal is: Get R0 down.
Here is the problem. R0 is an average. Misleading. Why? Consider a group of two. One is a millionaire. One is a pauper. There average income is $500,000. So – all is well?
Most people infected with COVID-19 do not spread it. A few spread it as super-spreaders. Why not focus on the super-spreaders? Why shut down everything, just to catch that handful of super-spreaders? “K” is a statistical measure of “dispersion” or “scatter” – do many people infect many others, or do a very few infect many others? Because, if it is the latter – then if we can find the super-spreaders, we can halt the spread, without disastrously shutting down the whole world!
And – how do you find the super-spreaders? Backward tracing. Conventionally, we trace forward. You have COVID-19? OK – with whom did you associate? And with whom did each of those associate?
Backward tracing means: Take a thousand persons infected in a given place. Work backward, to see who was it and where was it and when was it that they were infected? With the goal of finding that COVID-19 Mary – that super-spreader!
For example: At the Rose Garden ceremony introducing Judge Amy Barrett – who in the front row infected so many people, including the President, Hope Hicks, the campaign manager, and so many others? And most important – shut down mass events – like bars, weddings, and Trump rallies – that super-spread virus.
And now, the whole story.
= = = = =
The R mentioned in the daily press briefings represents an average of the whole country or region, involving millions of people. But its single value hides many differences between individuals and their impact on virus transmission.
Rather than assuming that every infected person and every contact they make follows the same pattern (as with the R number), scientists working on epidemic models allow for the number of new cases caused by each infected person to vary randomly. Some people might have high viral loads or might simply cough more and hence spread the virus more effectively. Many people, although ill and highly infectious, don’t show any symptoms. They might make many contacts without realising they pose a danger to others. An example from history is the infamous Mary Mallon (“Typhoid Mary”), a cook in New York City in the early 1900s. Although she carried typhoid bacteria, she didn’t show any symptoms and is believed to have infected more than 50 people over seven years.
Here is what Zeynep Tufekci writes:
“…. averages aren’t always useful for understanding the distribution of a phenomenon, especially if it has widely varying behavior. If Amazon’s CEO, Jeff Bezos, walks into a bar with 100 regular people in it, the average wealth in that bar suddenly exceeds $1 billion. If I also walk into that bar, not much will change. Clearly, the average is not that useful a number to understand the distribution of wealth in that bar, or how to change it. Sometimes, the mean is not the message. Meanwhile, if the bar has a person infected with COVID-19, and if it is also poorly ventilated and loud, causing people to speak loudly at close range, almost everyone in the room could potentially be infected—a pattern that’s been observed many times since the pandemic begin, and that is similarly not captured by R. That’s where the dispersion comes in. There are COVID-19 incidents in which a single person likely infected 80 percent or more of the people in the room in just a few hours. But, at other times, COVID-19 can be surprisingly much less contagious. Overdispersion and super-spreading of this virus are found in research across the globe. A growing number of studies estimate that a majority of infected people may not infect a single other person. A recent paper found that in Hong Kong, which had extensive testing and contact tracing, about 19 percent of cases were responsible for 80 percent of transmission, while 69 percent of cases did not infect another person. This finding is not rare: Multiple studies from the beginning have suggested that as few as 10 to 20 percent of infected people may be responsible for as much as 80 to 90 percent of transmission, and that many people barely transmit it.”
Notice this: It is the 80/20 rules so well known in management. 20% of the people do 80% of the work. 19% of the cases cause 80% of the transmission. So the goal has to be not R0 but K: FIND THOSE 19%!!! STOP THOSE MASS EVENT WHERE THE 19% ARE SPREADING VIRUS!.
OK. Prove it. So here is Japan’s approach based on “K”.
“Hitoshi Oshitani, a member of the National COVID-19 Cluster Taskforce at Japan’s Ministry of Health, Labour and Welfare and a professor at Tohoku University who told me that Japan focused on the overdispersion impact from early on, likens his country’s approach to looking at a forest and trying to find the clusters, not the trees. Meanwhile, he believes, the Western world was getting distracted by the trees, and got lost among them. To fight a super-spreading disease effectively, policy makers need to figure out why super-spreading happens, and they need to understand how it affects everything, including our contact-tracing methods and our testing regimes.
“In study after study, we see that super-spreading clusters of COVID-19 almost overwhelmingly occur in poorly ventilated, indoor environments where many people congregate over time—weddings, churches, choirs, gyms, funerals, restaurants, and such—especially when there is loud talking or singing without masks.”
And now – my country Israel. 28% of Ultra-Orthodox tested for coronavirus proved positive. Their lifestyle focuses on community prayer and celebration. Some 40% of all new cases come from this community, which is only a small fraction of the population.
Yet the whole country is locked down by the Prime Minister and cabinet. Why? To focus on the Ultra-Orthodox would be discriminatory, racist, anti-Semitic – and worst of all, politically damaging to the Prime Minister, who needs their votes and support, in his coalition.
So Israel’s “K” is small. We have superspreaders. But because of politics, we manage our policies based on R0. When Israel’s Project Manager for COVID-19 control, Dr. Roni Gamzu, mentioned the Ultra-Orthodox as super-spreaders, based on medical evidence, he was violently attacked and forced to apologize.
Sad.
So let us give Tufekci the last word – a word of hope. “Could we get back to a much more normal life by focusing on limiting the conditions for super-spreading events, aggressively engaging in cluster-busting, and deploying cheap, rapid mass tests—that is, once we get our case numbers down to low enough numbers to carry out such a strategy? (Many places with low community transmission could start immediately.) Once we look for and see the forest, it becomes easier to find our way out.”
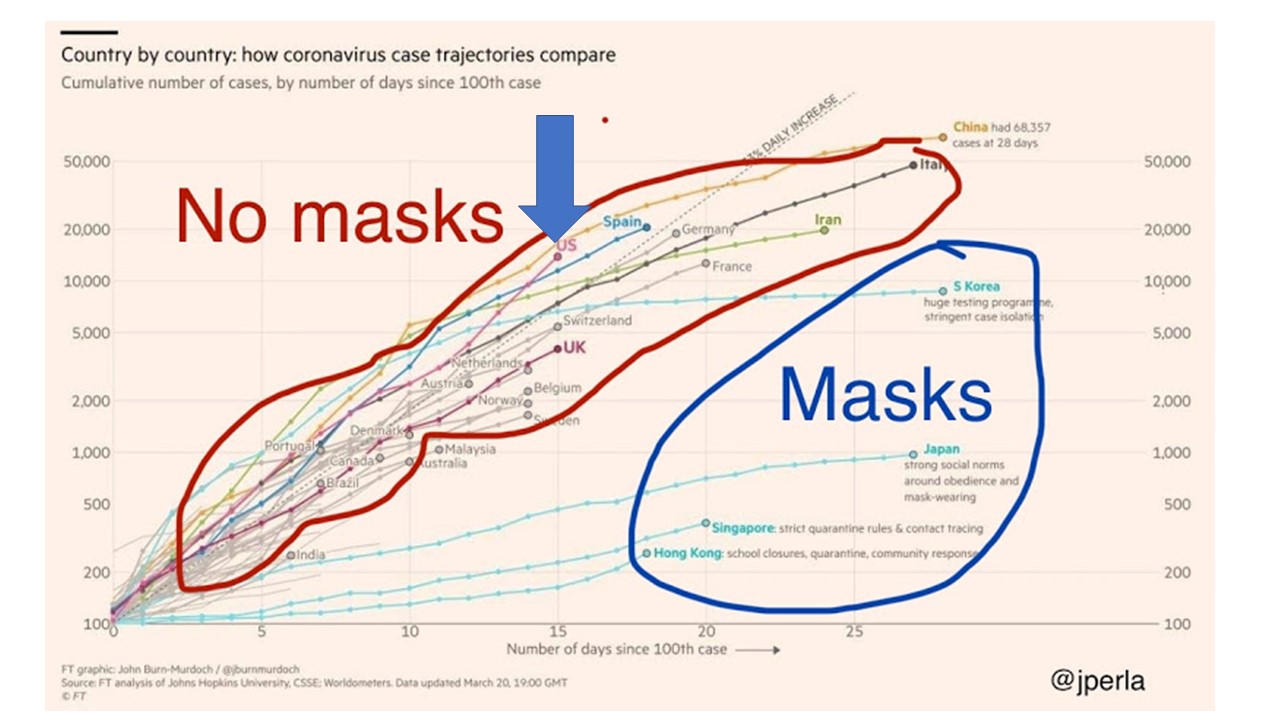
How to Save 40,000 Lives
By Shlomo Maital
OK – I am a very broken record. But I simply can’t get my mind around this one.
The Institute for Health Metrics & Evaluation, University of Washington, is perhaps one of the highest regarded credible sources of data and projections, related to the pandemic.
They have just completed a comprehensive study of data, regarding the impact of wearing facial masks. They not only read all the many studies – they re-analyzed the actual raw data.
Here are the results, just published.
Projected deaths from COVID-19 Under Three Scenarios, as of November 1: United States
Total Deaths Daily Deaths
- Easing, Opening 241,000 1,341
- Current Mix: Closed/Open 224,546 815
- Universal masks worn (95%) 183,242 273
How can the leader of the richest nation in the world live with himself, knowing that his public scorn of masks, and politicization of mask-wearing as an invasion of freedom (the freedom to die and to kill), will potentially kill 40,000 people – the total number of people who die in traffic deaths every year in the United States? Run the numbers: Easing and opening, return to schools, as the Administration wishes, versus universal mask wearing (and that, by the way, refers to ordinary cloth masks) kills 58,000 unnecessarily — and the current open/closed mix? 224,546 minus 183,242 equals over 40,000 superfluous deaths.
The IHME study shows conclusively that wearing a simple cloth mask, if everyone does, reduces the spread of COVID19 by 30%. That is a really big number. It could be the difference between an R0 number that creates a huge new wave, and an R0 number that gradually extinguishes the virus.
POTUS. A one-man death squad, aided by some Neanderthal southern governors.
Mission Accomplished? Uh, Whoops, Not Quite!
By Shlomo Maital
Bush’s Mission Accomplished speech
A small bit of 17-year-old history: In his “Mission Accomplished” speech (named for a banner displayed above the speaker) United States President George W. Bush spoke on the aircraft carrier USS Abraham Lincoln on May 1, 2003. Bush stated it was the end to major combat operations in Iraq. We won. Yay!
Bush’s claim —and the sign itself—became controversial after warfare in Iraq increased during the Iraqi insurgency. The vast majority of casualties, both military and civilian, occurred after the speech.
Fast forward. In the Wall Street Journal, Vice-President Mike Pence declares, just two weeks ago: “There Isn’t a Coronavirus ‘Second Wave’. With testing, treatments and vaccine trials ramping up, we are far better off than the media report.” Meanwhile, the US is among world leaders with some 50,000 new cases daily. And President Trump? CNN reports: in mid June, “ when U.S. health officials reported nearly 27,000 new Covid-19 cases, President Trump said in a television interview that the virus was “dying out.” He brushed off concerns about an upcoming rally in Tulsa, Okla., because the number of cases there is “very miniscule,” despite the state’s surging infection rate.”
Mission Accomplished? A victory lap? Not quite. And people are dying as a result.
My country Israel is no exception. We are among world leaders in new cases per 1,000 population. And the numbers are rising. A bloated coalition cabinet is like a carving I once saw, a two headed snake, one head trying to eat the other. This, after our Prime Minister took ‘credit’ for Israel’s astounding success in defeating the coronavirus.
And it is no second wave. It is the continued first wave, of a sneaky wily piece of ribonucleic acid that is humiliating the vaunted brainpower of humans, 86 billion brain cells for each of the 8 billion or so people on earth. Two to zero, in favor of the virus.
No, mission not accomplished. And the arrogance of claiming that it is, is itself criminal.
Remdesivir: Grasping at Straws!
By Shlomo Maital

There is a massive amount of fake news circulating now about COVID-19, some of it racist, pernicious and dangerous. There is also well-meaning news, reports that want to bring hope but in fact are simply grasping at straws.
A report now viral, emanating from the University of Chicago, is about how an anti-viral drug developed by a pharma company, Gilead, has helped seriously ill COVID-19 patients.
Remdesivir is an antiviral medication; a nucleotide analog, specifically an adenosine analogue, which inserts into viral RNA chains, causing their premature termination. It is being studied during 2020 as a possible post-infection treatment for COVID-19 illness.
A U of Chicago doctor participated in an internal hospital video in which she reported that when seriously ill patients administered remdesivir, many recovered.
The video reached some hospital employees, who leaked it to journalists. That led to a highly optimistic report.
This is not a clinical test. There is no protocol, and no placebo (sugar pill given to some patients).
The drug, made by Gilead Sciences, was tested against Ebola with little success, but multiple studies in animals showed the drug could both prevent and treat coronaviruses related to Covid-19, including SARS (Severe Acute Respiratory Syndrome) and MERS (Middle East Respiratory Syndrome).
We are all desperate for some good news. But grasping at straws is not going to help. The journalists who reported this “scoop” should have told us exactly what the source was, an internal chatty ‘gossip’ video of the kind that circulates in most hospitals.
The journalist who DID inform us was the CNN medical correspondent, is Elizabeth Cohen, who has serious training and deep scientific knowledge. She has a Master’s degree in public health. Her colleague is Dr. Sanjay Gupta, a neurosurgeon; together they comprise “the horse’s mouth” and to mix a metaphor, a horse’s mouth that does NOT grasp at straws.
A Vaccine is Coming – from Pittsburgh
By Shlomo Maital

Univ. of Pittsburgh “Cathedral of Learning”
Before the good news about a COVID-19 vaccine – a piece of history.
In 1947, native New Yorker Jonas Salk accepted an appointment to the University of Pittsburgh School of Medicine. In 1948, he undertook a project funded by the National Foundation for Infantile Paralysis to determine the number of different types of poliovirus. Salk saw this was a golden opportunity to extend this project towards developing a vaccine against polio. He built a research team and devoted himself to this work for the next seven years. The field trial set up to test the Salk vaccine involved 20,000 physicians and public health officers, 64,000 school personnel, and 220,000 volunteers. Over 1.8 million schoolchildren took part in the trial.
On March 26, 1953, Salk announced on a national radio show that he had successfully tested a vaccine against poliomyelitis, the virus that causes the crippling disease of polio. In 1952—an epidemic year for polio—there were 58,000 new cases reported in the United States, and more than 3,000 died from the disease. Dr. Salk was celebrated as the great doctor-benefactor of his time.
Fast forward. A press release from the NIH: https://www.nih.gov/news-events/nih-research-matters/microneedle-coronavirus-vaccine-triggers-immune-response-mice
“After the identification of SARS-CoV-2, the genome sequence of the new coronavirus was rapidly released to the public by scientists in China. Several weeks later, National Institute of Health-funded scientists produced a detailed picture of the part of the virus, called the spike protein, that allows it to infect human cells. This spike protein is currently the target of several vaccine development efforts. And we see the graphic version of the corona ‘spikes’ everywhere…
“Researchers led by Drs. Louis Falo, Jr. and Andrea Gambotto from the University of Pittsburgh have been working to develop vaccines for other coronaviruses, including the one that causes Middle East Respiratory System (MERS). They adapted the system they had been developing to produce a candidate MERS vaccine to rapidly produce an experimental vaccine using the SARS-CoV-2 spike protein.
The team developed a method for delivering their MERS vaccine into mice using a microneedle patch. Such patches resemble a piece of Velcro, with hundreds of tiny microneedles made of sugar. The needles prick just into the skin and quickly dissolve, releasing the vaccine. Since the immune system is highly active in the skin, delivering vaccines this way may produce a more rapid and robust immune response than standard injections under the skin.
“When delivered by microneedle patch to mice, three different experimental MERS vaccines induced the production of antibodies against the virus. These responses were stronger than the responses generated by regular injection of one of the vaccines along with a powerful immune stimulant (an adjuvant). Antibody levels continued to increase over time in mice vaccinated by microneedle patch—up to 55 weeks, when the experiments ended.
“Using knowledge gained from development of the MERS vaccine, the team made a similar microneedle vaccine targeting the spike protein of SARS-CoV-2. The vaccine prompted robust antibody production in the mice within two weeks.
“The vaccinated animals haven’t been tracked for enough time to see if the long-term immune response is equivalent to that observed with the MERS vaccines. The mice have also not yet been challenged with SARS-CoV-2 infection. However, the findings are promising in light of results from the similar MERS vaccine.
“The components of the experimental vaccine could be made quickly and at large-scale, the researchers say. The final product also doesn’t require refrigeration, so it could be produced and placed in storage until needed. The team has now begun the process of obtaining approval from the U.S. Food and Drug Administration to launch a phase 1 trial within the next several months.
“Much work still needs to be done to explore the safety and efficacy of this candidate vaccine. “Testing in patients would typically require at least a year and probably longer,” Falo says. “This particular situation is different from anything we’ve ever seen, so we don’t know how long the clinical development process will take.”
OK – it works in mice. Now for humans. A vaccine is on the way – and it may emerge again from Univ. of Pittsburgh.
What Do We NOT Know?!
By Shlomo Maital

After more than four months of nonstop news/debate/discussion around COVID-19, it is astonishing how much we do not know. And as the saying goes, what you don’t know that you don’t know — is the worst; it can literally kill you.
So here is my attempt to list, what it is we don’t know, that we NEED to know, about this tiny virulent enemy and hopefully, scientists are working on it.
- For those who get COVID-19 and recover, are they immune? For life? For a short time? How long does the immunity last?
- Like many viruses, can this novel coronavirus mutate quickly and attack those who contracted an older version? Are COVID-19 cases in the US characterized by the same genetically-identical virus as say in China, or different? If so, how different? And does it matter?
- Intubation: Are we in too much of a hurry to put people on intubation (ventilators)? If such a small percentage of those intubated, survive, should we rethink this? And how different are the various kinds of ventilators (those used by anesthetists, oxygen ventilators, standard ventilators, etc.)?
- Why are the death rates (those who die from COVID-19, as a % of those who are seriously ill, or in general % of those who contract the virus) different, radically, between one country and another? How much of this is due to ICU expertise?
- How exactly does COVID-19 spread? As aerosol (tiny droplets that hang in the air for hours?) As big droplets (that fall to the ground fairly quickly)?
- Are there drugs proven to be effective against COVID-19? What about the recently-approved anti-influenza drugs? Xofluza, Tamiflu, Relenza, Rapivab ? And, of course, hydroxychloroquine? (which seems to have severe heart side-effects among some patients).
- Why are African-Americans more afflicted than Caucasians? Men more than women?
- Will there be a second wave? And a third? How will we know in time?
- How soon will we have a proven vaccine, and how quickly can doses be produced, to inoculate billions of people? How much will it cost? Can it be provided for free? How can the many companies working on a vaccine, in many countries, work together, to save time and save lives?
- What countries have managed the COVID-19 crisis best, and what can be learned from them? There have been many variations on lockdown, ranging from easy (Sweden) to draconian (China, Singapore). Which works best?
- Somewhere, as we speak, a new virus is brewing and mutating somewhere; this is not the last pandemic. Can we organize a world-spanning organization (broader in span than WHO, with far more resources) that will be ready to tackle the next pandemic quickly and efficiently? With massive resources?
I’m certain there are a thousand more things we do not know. Add your own questions… for each question above, there are multiple answers online, and many of them are fake or conspiratorial. This simply adds to the fog.
COVID-19: Who’s In Charge? And Who Should Be in Charge?
By Shlomo Maital

OK – who’s in charge? Who is running the coronavirus pandemic show?
I think it’s pretty obvious – it’s the doctors, medical experts, epidemiologists and public health officials. As it should be. Right?
No, I’m not so sure. Initially the focus worldwide was on stopping the spread of COVID-19 from China to the world. That pretty much failed, as expected – with millions of people travelling every week, and with some countries reluctant to share information, drastic quarantine measures came a bit too late. And now, COVID-19 is in some 70-80 countries. So – it has spread. Now what?
Public health officials are in charge. And lacking medicine or vaccines, their tool is mainly that of quarantine. In Israel, a small country, with very few causes of new coronavirus, some 100,000 people are in self-imposed quarantine, for 2 weeks, largely because they have been in countries like France and Italy, where coronavirus existed.
Quarantine may be rather ineffective in halting the infectious spread. And it is disastrous for the economy. You cannot simply shut down the world economy – people have to eat and drink and keep the wheels of commerce moving. It cannot really be done efficiently from home… the Internet is not yet up to it.
So who is running the show? What we need is a small, powerful interdisciplinary team made up of political leaders, public health experts, epidemiologists, and yes, perhaps economists, and psychologists, and information experts, who will focus on the system – the big picture. How to deliver accurate information. (America gets a big ‘F’ on this one, largely due to its President, who brags that he is terrific at numbers and maybe should have been a doctor rather than an amateur politician). How to weigh cost-benefit in quarantine policies. How and when and whom to test for COVID-19. How to deal with public transportation and flights. How to run schools.
You could in principle simply shut everything down and tell everyone to stay home. That would be disastrous, immensely costly, and harmful to the mental health of the nation. I don’t believe this is an option. So the question is, how to keep things running more or less smoothly, in the face of the coronavirus that is here to stay? For hat we need a systems approach.
This is all new territory. We have not faced a real pandemic, post-1989 global economy. Each country needs an integrated team to make policy, and the world needs a similar integrated team to coordinate policies among nations.
Perhaps, if something good will emerge from the COVID-19 crisis, it will be the understanding of how interdependent all of us are, everywhere, and how concrete and steel walls are not the answer.
My Two Key Skills: What are Yours?
By Shlomo Maital

Qwerty keyboard on an old Underwood typewriter
After writing magazine columns on our failing schools, I reflected on what I myself learned in school.
The two key skills I learned? In high school, Grade 9 – touch typing. I learned to type very fast, 80 words a minute, owing to strong incentives to do boring exercises again and again. This turned out to be a crucial skill. I was able to put my thoughts on to paper very rapidly, as I could type almost as fast as I could speak. Probably, in another life, I would have chosen to be a journalist rather than an economist. That skill that I learned in 1956 has served me well for 63 years. I even worked one summer as a typist, typing invoices — I can touch-type numbers very fast, too.
Note: I still have my mother’s old Underwood typewriter, with the QWERTY keyboard, designed so that the keys, operated by spring mechanisms, should not clash and tangle with one another… Qwerty is still the standard, even though typing has long since been digital – showing the inertia of human behavior. My late mother worked as a typist for the Provincial Government, Dept. of Agriculture, in Regina, Saskathewan; I’m forever grateful she urged me to learn touch typing.
The second key skill I learned was as a freshman in college, at Queen’s University, Kingston Ontario. All freshmen in Arts & Science, in those days, had to take Philosophy 1, given by A.R.C. Duncan, a Scottish philosopher of the old school. It was a tough rigorous course, covering the 3 branches of Philosophy – ethics, metaphysics and logic. I learned critical thinking, how to fashion a logical argument, what the various approaches to right and wrong are….. memorable, and something I use daily.
I fear today’s young people do not have the same privilege, and do not acquire crucial critical thinking skills.
….
Dear reader: What, on reflection, did YOU learn in school, that turned out to be supremely valuable and relevant?
Paul Volcker, 1927-2019: How He Saved the World from Inflation
By Shlomo Maital

Paul Volcker 1927-2019
Paul Volcker has passed away; he was 92. Volcker served as Chair of the Federal Reserve Bank, appointed by Jimmy Carter in 1979.
Volcker was a giant, physically, standing 6 ft. 7 inches tall – but also a giant in wisdom and courage. The US was afflicted by double digit inflation, from 1979 to 1981, driven by cost-push price rises and soaring oil prices. Volcker quickly understood the threat. With the dollar serving as the world’s major, perhaps only, globally-accepted currency, US inflation threatened not only the US but also the global trading system, then struggling from recessions in 1973 and again in 1978/9.
Volcker acted with what then seemed like outrageous boldness. He raised Fed interest rates to 21%. This was unheard of. I can only imagine what today’s President, Donald J. Trump, would have said, had he (heaven forbid) have been president at that time. Trump wants zero interest rates, no matter what the economy needs, and has hassled current Fed Chair Jerome Powell over his unwillingness to promote cheap credit at all cost and at all times.
Volcker’s move put a halt to the inflation, stopping it in its tracks, but also ground the economy to a halt, causing a recession, or what came to be known as stagflation. Partly as a result Jimmy Carter became a one-term President, defeated in November 1980 by Ronald Reagan. It was ironic that Carter lost partly because of a very wise and strong appointment that he made, to the Fed.
We must remember Volcker and the strong independence of the Federal Reserve system that prevailed, until now. No President has dared messing with the Fed’s independence, until now. Research shows that nations with strong independent central banks fare far better than those where governments make their central banks into private money-printers. Trump endangers today’s Fed, and as a result, endangers the world. We should remember Volcker fondly, and recall the lesson he taught us.

