The Race to a COVID-19 Vaccine: Q&A
By Shlomo Maital

Where do we stand in the quest for a safe effective COVID-19 vaccine?
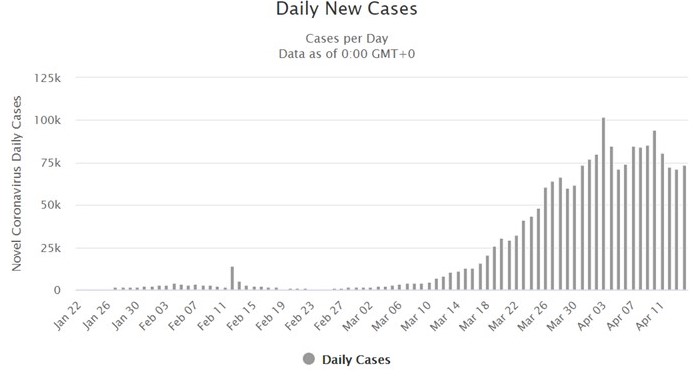
More than 2.2 million persons worldwide have contracted the virus and of those, 154,783 have died. That is a 6.8% death rate. But wait – there are far far more cases worldwide than those we know about. Deaths are certain; cases are a guess. If we use a 1% to 1.5% death rate, we can guess that between 10 million and 15 million persons worldwide have contracted the illness. Only an effective vaccine will put a clear end to this crisis, in which COVID-19 is already the #1 cause of death in the US.
This Q&A is based on an informative survey published in a reputable website, livescience.com, by staff writer By Nicoletta Lanese, two days ago: (Warning: this blog is long, 1895 words…sorry).
* https://www.livescience.com/coronavirus-covid-19-vaccine-timeline.html
When will a vaccine be ready?
“Here’s why it probably can’t be developed any sooner than 12 to 18 months.
“More than 60 candidate vaccines are now in development, worldwide, and several have entered early clinical trials in human volunteers, according to the Some groups aim to provoke an immune response in vaccinated people by introducing a weakened or dead SARS-CoV-2 virus, or pieces of the virus, into their bodies. The vaccines for measles, influenza, hepatitis B and the vaccinia virus, which causes smallpox, use these approaches, according to the U.S. Department of Health & Human Services. Although tried-and-tested, using this approach to develop these conventional vaccines was labor-intensive, requiring scientists to isolate, culture and modify live viruses in the lab.
That initial process of just creating a vaccine can take 3 to 6 months, “if you have a good animal model to test your product,” Raul Andino-Pavlovsky, a professor in the Department of Microbiology and Immunology at the University of California, San Francisco, told Live Science. “
Are there short cuts? How fast is the US working on a vaccine?
“The first COVID-19 vaccine to enter clinical trials in the United States, for example, uses a genetic molecule called mRNA as its base. Scientists generate the mRNA in the lab and, rather than directly injecting SARS-CoV-2 into patients, instead introduce this mRNA. By design, the vaccine should prompt human cells to build proteins found on the virus’ surface and thus trigger a protective immune response against the coronavirus. Other groups aim to use related genetic material, including RNA and DNA, to build similar vaccines that would interfere with an earlier step in the protein construction process. But there’s one big hurdle for mRNA vaccines. We can’t be sure they will work. As of yet, no vaccine built from a germs’ genetic material has ever earned approval, Bert Jacobs, a professor of virology at Arizona State University and member of the ASU Biodesign Institute’s Center for Immunotherapy, Vaccines and Virotherapy, told Live Science. Despite the technology having existed for almost 30 years, RNA and DNA vaccines have not yet matched the protective power of existing vaccines, National Geographic reported.
In this high-stakes competition, is there also collaboration?
“Assuming these unconventional COVID-19 vaccines pass initial safety tests, “will there be efficacy?” Jacobs said. “The animal models suggest it, but we’ll have to wait and see.” “Because of the emergency here, people are going to try many different solutions in parallel,” Andino-Pavlovsky said. The key to trialing many vaccine candidates at once will be to share data openly between research groups, in order to identify promising products as soon as possible, he said.
Could a COVID-19 vaccine be potentially dangerous and do damage?
For sure.
“Designing a vaccine that grants immunity and causes minimal side effects is no simple task. A coronavirus vaccine, in particular, poses its own unique challenges. Although scientists did create candidate vaccines for the coronaviruses SARS-CoV and MERS-CoV, these did not exit clinical trials or enter public use, partly because of lack of resources, Live Science previously reported. “One of the things you have to be careful of when you’re dealing with a coronavirus is the possibility of enhancement,” Fauci said in an interview with the journal JAMA on April 8. Some vaccines cause a dangerous phenomenon known as antibody dependent enhancement (AED), which paradoxically leaves the body more vulnerable to severe illness after inoculation. Candidate vaccines for dengue virus, for example, have generated low levels of antibodies that guide the virus to vulnerable cells, rather than destroying the pathogen on sight, Stat News reported. Coronavirus vaccines for animal diseases and the human illness SARS triggered similar effects in animals, so there’s some concern that a candidate vaccine for SARS-CoV-2 might do the same, according to an opinion piece published March 16 in the journal Nature. Scientists should watch for signs of AED in all upcoming COVID-19 vaccine trials, Fauci said. Determining whether enhancement is occurring could happen during initial animal studies, but “it is still unclear how we will look for AED,” Jacobs said.
Are there specific dangers in developing a COVID-19 vaccine?
A successful coronavirus vaccine will snuff the spread of SARS-CoV-2 by reducing the number of new people infected, Andino-Pavlovsky said. COVID-19 infections typically take hold in so-called mucosal tissues that line the upper respiratory tract, and to effectively prevent viral spread, “you need to have immunity at the site of infection, in the nose, in the upper respiratory tract,” he said. These initial hotspots of infection are easily permeated by infectious pathogens. A specialized fleet of immune cells, separate from those that patrol tissues throughout the body, are responsible for protecting these vulnerable tissues. The immune cells that protect mucosal tissue are generated by cells called lymphocytes that remain nearby, according to the textbook “Immunobiology: The Immune System in Health and Disease” (Garland Science, 2001).
“It’s like your local police department,” Andino-Pavlovsky told Live Science. But not all vaccines prompt a strong response from the mucosal immune system, he said. The seasonal influenza vaccine, for example, does not reliably trigger a mucosal immune response in all patients, which partly explains why some people still catch the respiratory disease after being vaccinated, he said.
“Even if a COVID-19 vaccine can jumpstart the necessary immune response, researchers aren’t sure how long that immunity might last, Jacobs added. While research suggests that the coronavirus doesn’t mutate quickly, “we have seasonal coronaviruses that come, year in [and] year out, and they don’t change much year to year,” he said. Despite hardly changing form, the four coronaviruses that cause the common cold keep infecting people — so why haven’t we built up immunity?
Could the COVID-19 virus pose special problems?
“Perhaps, there’s something odd about the virus itself, specifically in its antigens, viral proteins that can be recognized by the immune system, and that causes immunity to wear off. Alternatively, coronaviruses may somehow fiddle with the immune system itself, and that could explain the drop-off in immunity over time, Andino-Pavlovsky said. To ensure a vaccine can grant long-term immunity against SARS-CoV-2, scientists will have to address these questions. In the short term, they’ll have to design experiments to challenge the immune system after vaccination and test its resilience through time, Jacobs said. In a mouse model, such studies could take “at least a couple of months,” he said. Scientists cannot conduct an equivalent experiment in humans, but can instead compare natural infection rates in vaccinated people to those of unvaccinated people in a long-term study. “When you have the luxury, you look at this for five years, 10 years to see what happens,” Andino-Pavlovsky added.
How will they ensure that a COVID-19 vaccine is safe?
“Unlike an antiviral treatment for COVID-19 that can be given to patients already infected with the virus, a vaccine must be tested in diverse populations of healthy people. “Because you give it to healthy people, there’s an enormous pressure to make sure it’s absolutely safe,” Andino-Pavlovsky said. What’s more, the vaccine must work well for people of many ages, including the elderly, whose weakened immune systems place them at heightened risk of serious COVID-19 infection. “Initially, safety studies will be done in small numbers of people,” likely fewer than 100, Jacobs said. A vaccine may be approved based on these small studies, which can take place over a few months, and then continually monitored as larger populations become vaccinated, he added. “That’s just my guess.”
[Note: The high and growing death toll from COVID-19 may justify some speed-up and short-cuts].
So what are the various stages that a vaccine must undergo, before it can be mass produced?
“Any potential vaccine will need to pass a safety trial, known as a Phase 1 trial, which also helps determine the needed dose. The next step is a larger trial in 100 to 300 people, called a Phase 2, which looks for some biological activity, but can’t say for sure if the drug is effective. If a vaccine candidate prompts a promising immune response in Phase 2 clinical trials, after passing safety tests in Phase 1, it’s possible that the FDA could approve such a vaccine for emergency use “before the 18-month period that I said,” Fauci said in the JAMA interview. “If you get neutralizing antibodies,” which latch onto specific structures on the virus and neutralize it, “I think you can keep moving forward on it,” Jacobs said. Normally, a vaccine would then enter Phase 3 clinical trials, which include hundreds to thousands of people.
“So adding up these steps, each of which will likely take 3 to 6 months, it’s very unlikely we would be able to find a vaccine that is safe and effective in less than 12 months — even if many of these steps could be done in parallel.
Can it be mass-produced? How?
“Then comes the issue of manufacturing billions and billions of doses of a new vaccine whose ingredients we don’t yet know. Bill Gates has said that the Gates Foundation will fund the construction of factories for seven coronavirus vaccine candidates, equipping the sites to produce a wide variety of vaccine types, Business Insider reported.
[Neanderthal Conservative groups have attacked Gates, making false and inflammatory claims about him].
“Even though we’ll end up picking at most two of them, we’re going to fund factories for all seven, just so that we don’t waste time in serially saying, ‘OK, which vaccine works?’ and then building the factory,” Gates said. Even if a fairly promising vaccine surfaces by 2021, and can be mass-produced, the search won’t end there. “Especially with trying to get something out this quickly, we may not get the best vaccine out there right away,” Jacobs said. Ideally, an initial vaccine will grant immunity for at least one to two years, but should that immunity wane, a longer lasting vaccine may have to be deployed. Historically, so-called live attenuated vaccines that contain a weakened virus tend to perform most reliably over extended periods of time, Andino-Pavlovsky said.
“That may be what we need in the long run,” he said. And research into coronavirus immunity should continue, regardless, “not only for COVID-19, but for the next coronavirus that comes.