
You are currently browsing the tag archive for the ‘coronavirus’ tag.
COVID-19: Plasma DOES Help!
By Shlomo Maital

Plasma is a component of our blood. Some 44% of our blood comprises red cells (that carry oxygen to and from the heart and the lungs and other organs), 1% are white blood cells that fight ‘invaders’, and 55% is plasma. It is the liquid part of the blood that carries cells and proteins throughout the body.
There is a theory that plasma from patients who have had COVID-19 and recovered contain antibodies, that can be helpful for other patients in overcoming the illness – especially those who are very seriously ill.
Research in Israel has provided serious confirmation. For those who are very seriously ill with COVID-19, many of them elderly with other serious preconditions, some 50% or so do not recover. When they are administered plasma, that contains antibodies generated by the body to fight the virus, drawn from recovered patients, he rate of recovery improves from about half to one-third, 33%.
Many Israelis have volunteered to donate plasma, after recovering – especially among the ultra-Orthodox community, which has been heavily afflicted by COVID-19.
Israel now has a special plasma bank, with many doses of such plasma, in the event that there is a second wave of the virus. Meanwhile, on May 18, there were only 16 new cases, and two deaths. In total Israel has suffered 278 deaths from COVID-19, a relatively low number, out of some 17,000 cases; of those, 13,435 have fully recovered. Only 50 persons remain in critical condition, on ventilators.
Kerala and KK Shailaja Show the Way!
By Shlomo Maital

KK Shailaja, Kerala Health Minister
On Jan. 21: The first case of the coronavirus is confirmed in the United States, in Seattle.
On Jan. 22: Trump makes his first comments about the coronavirus, saying he is not concerned about a pandemic: “No. Not at all. And we have it totally under control. … It’s going to be just fine.”
Contrast this with the Health Minister of Kerala, K.K. Shailaja, a former teacher. (She is known affectionately as Shailaja Teacher). Kerala is a state in southwest India, with some 35 million people, and its population is quite highly educated; its politics are socialist and, let’s say it, Communist.
According to a fine article in The Guardian by Laura Spinney:
“On 20 January, KK Shailaja phoned one of her medically trained deputies. She had read online about a dangerous new virus spreading in China. “Will it come to us?” she asked. “Definitely, Madam,” he replied. And so the health minister of the Indian state of Kerala began her preparations. Four months later, Kerala has reported only 524 cases of Covid-19, four deaths and – according to Shailaja – no community transmission. The state has a population of about 35 million and a GDP per capita of only £2,200. By contrast, the UK (double the population, GDP per capita of £33,100) has reported more than 40,000 deaths, while the US (10 times the population, GDP per capita of £51,000) has reported more than 82,000 deaths; both countries have rampant community transmission.
What does Shailaja Teacher and Kerala understand, that President Trump does not?
The Guardian continues: “Three days after reading about the new virus in China, and before Kerala had its first case of Covid-19, Shailaja held the first meeting of her rapid response team. The next day, 24 January, the team set up a control room and instructed the medical officers in Kerala’s 14 districts to do the same at their level. By the time the first case arrived, on 27 January, via a plane from Wuhan, the state had already adopted the World Health Organization’s protocol of test, trace, isolate and support. As the passengers filed off the Chinese flight, they had their temperatures checked. Three who were found to be running a fever were isolated in a nearby hospital. The remaining passengers were placed in home quarantine – sent there with information pamphlets about Covid-19 that had already been printed in the local language, Malayalam. The hospitalised patients tested positive for Covid-19, but the disease had been contained. “The first part was a victory,” says Shailaja. “But the virus continued to spread beyond China and soon it was everywhere.” In late February, encountering one of Shailaja’s surveillance teams at the airport, a Malayali family returning from Venice was evasive about its travel history and went home without submitting to the now-standard controls. By the time medical personnel detected a case of Covid-19 and traced it back to them, their contacts were in the hundreds. Contact tracers tracked them all down, with the help of advertisements and social media, and they were placed in quarantine. Six developed Covid-19.”
Spinney observes: “ The Communist Party of India (Marxist), of which she is a member, has been prominent in Kerala’s governments since 1957, the year after her birth. (It was part of the Communist Party of India until 1964, when it broke away.) Born into a family of activists and freedom fighters – her grandmother campaigned against untouchability – she watched the so-called “Kerala model” be assembled from the ground up; when we speak, this is what she wants to talk about.”
Trump vilifies socialism without understanding what it is, calls the Democrats ‘socialists’, and his sycophants caution against becoming “like Denmark” (a society and economy far more equitable, healthy and unified than the US). Imagine what Trump would say about Kerala, if he knew where India was on the map or what Shailaja Teacher had done.
How many people died, because Trump leads the US and not Communist Shailaja? How many lives could have been saved, had Trump acted weeks or even days sooner?
And will voters rightly fix the blame on his shoulders, on November 3, in the US?
Postscript: One of the world’s leading medical journals is The Lancet. Read The Lancet’s unprecedented Editorial, showing how Trump gutted the Center for Disease Control (CDC), politicized it, and made it unable to deal properly with the COVID-19 crisis. No-one can remember the last time when a scientific journal like the Lancet has editorialized so fiercely.
[Special thanks to Pramod Arikal, my former student, for drawing my attention to this important story].
Leadership: Give the Keys to Young Educated Women
By Shlomo Maital

Of some 200 countries in the world – which have had leaders most competent and successful in leading responses to the pandemic?
Let’s begin with the losers. Aging autocratic poorly-educated men, in denial, who missed the boat. The ‘orange haired narcissist’, as NYT columnist Roger Cohen calls him, Donald J. Trump. The whacko Brazilian president Jair Bolsinaro, possibly facing impeachment (like his mentor Trump). “So what?” was his response, when asked about Brazil’s death toll, highest in South America. Vladimir Putin, who cowardly shelters and lets others take the blame. Erdugan, who despite the crisis pursues his foes with paranoid insanity.
And now for the winners. Young educated women. 39-year-old Jacinda Ardern, who saw what was happening and shut down New Zealand with only 53 proven cases. Finland’s Prime Minister Sanna Marin, 34, one of the youngest political leaders in the world. Norway’s Prime Minister Erna Solberg. (She’s 59, tough, “Iron Erna”, and young in spirit). And never forget German Chancellor Angela Merkel – not young, like the others, but educated, a scientist, and quietly compassionate and competent. In Iceland, Katrin Jacobsdottir, 44, who organized free COVID-19 testing for all! And don’t forget Taiwanese President Tsai Ing-Wen, 64.
Now, a Yiddish saying goes, “for instance is not a proof”. But a spate of terrific female Prime Ministers who have led their country with bravery courage and excellence – this is not an accident, in the face of aging despot men who have utterly failed.
So suppose the world was a locked house, with a set of keys. Who should get the keys? Smart competent women, who have fought their way up the political ladder against all the odds. Educated women, who speak well, do their homework, listen to experts, and win the trust of their people. Compassionate women, who understand human suffering and communicate this compassion.
And the despotic men? As Trump loves to say, “lock ‘em up”. Fast. Before it’s too late. Figuratively, of course – at the ballot box. Tuesday Nov. 3, 2020, a crucial date for the US and the world. Bye bye, orange-haired narcissist. Hello, Democrat female educated courageous well-spoken Vice President. And future President.
Does the Novel Coronavirus Mutate?
By Shlomo Maital

Writing in today’s New York Times, Nathaniel Lash and Tala Schlossberg try to answer the key question, does the novel coronavirus mutate? If so, how and when?
Here is why it is important for us to know this. The pandemic crisis will end only when we have a vaccine, produced in billions of doses. The vaccine will work by stimulating the body to produce antibodies that neutralize the virus by binding to it in a very specific way. If the virus can mutate to defeat the vaccine, then the vaccine will not stop working. The key is the “spike protein” – the protein the virus makes that penetrates the cell walls and lets the virus invade (and kill) it. Those are the spikes you see in the graphic illustrations of corona. Vaccines can defeat the spike.
Here is what the authors of the article have found:
“Among the thousands of samples of the long strand of RNA that makes up the coronavirus, 11 mutations have become fairly common. But as far as we know, it’s the same virus infecting people all over the world, meaning that only one “strain” of the virus exists, said Peter Thielen, a molecular biologist with the Johns Hopkins Applied Physics Laboratory. Only one of those common mutations affects the “spike protein,” which enables the virus to infect cells in the throat and lungs. Efforts to produce antibodies that block the spike protein are central to many efforts to develop a vaccine. Since the spike protein has changed little so far, some scientists believe that’s a sign that it can’t alter itself very much and remain infectious.”
So – we have a small piece of good news. The measles vaccine, for instance, was developed in 1950. And it is still effective. Measles hasn’t mutated in a manner that neutralizes the vaccine. Evolution is powerful – but apparently it cannot surmount EVERY obstacle. So hopefully the same will apply to the COVID-19 vaccine – and we will bid this insidious deadly enemy good-bye, with an effective vaccine… until the next one.
The End of the Beginning
By Shlomo Maital
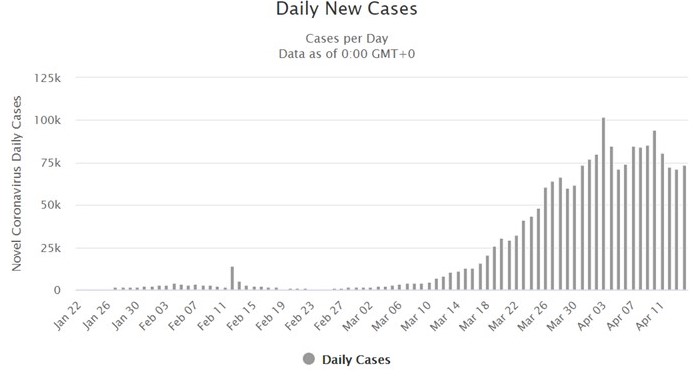
There is evidence that, to quote Winston Churchill, “we are not at the beginning of the end, but..at the end of the beginning.” Here are the daily totals of new cases worldwide, thanks to worldometer.com, and next to them, the % daily change:
| 3-Apr | 101736 | |
| 4 | 84821 | -16.6 % |
| 5 | 71502 | -15.7 |
| 6 | 74044 | 3.6 |
| 7 | 85116 | 15.0 |
| 8 | 84447 | -0.8 |
| 9 | 85638 | 1.4 |
| 10 | 94629 | 10.5 |
| 11 | 80963 | -14.4 |
| 12 | 72523 | -10.4 |
| 13 | 71572 | -1.3 |
| 14 | 73969 | 3.3 |
What this looks like, is a kind of ‘plateau’ levelling off — as the coronavirus spread globally, some countries were afflicted early, others later. So countries will reach their ‘apex’ at differing times… (the US is still not there yet)…. And this will produce a kind of plateau worldwide.
The reason this is important, is this — countries will begin to emerge from their ‘lockdown’ at different times, some sooner than others. Denmark is opening its kindergartens, China is sending Wuhan back to work in part.
But in terms of public health, we need to see this as a global system. If there are hot pockets in one country, no country is safe – because a return to normality will restart flights and travel. And we still do not fully understand the duration or extent of coronavirus immunity for those who had it.
How to Emerge from Lockdown: Speed is Vital!
By Shlomo Maital
Question: how does coronavirus resemble standup comedy?
Answer: For both, timing is crucial.
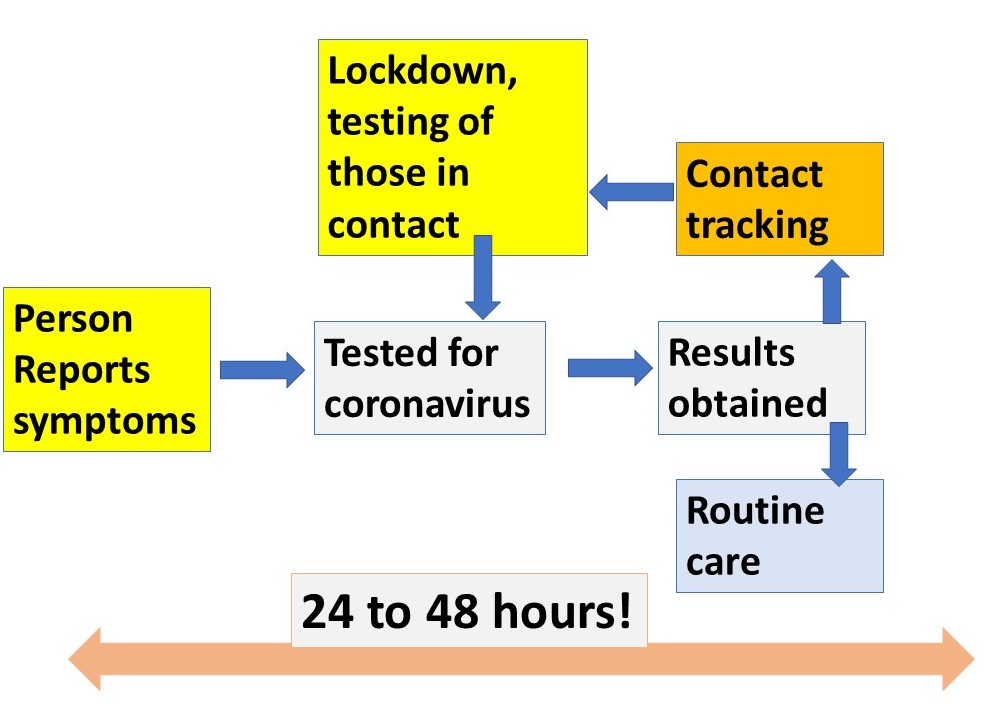
As countries begin to emerge from lockdown (Denmark has opened its kindergartens, because 90% of families with children have both parents working), fears arise whether this is wise. One answer is, yes, but… The diagram above shows how emergence can best be done. And everything, EVERYthing, depends on timing and speed —
- test for virus among those with symptoms, and some who are asymptomatic,
- get the results super-fast, within hours (this is possible with some tests),
- track those in contact with persons testing positive,
- lock down those with the virus, and
- do this again and again.
All this depends on revising current testing procedures (some results have been lost, some take 6-8 days for results, far too long to be useful). Timing and speed are crucial. Why? Because, in the 6 days it takes now for results to be provided, the person potentially infected can infect many many other people, even unknowingly.
Does your country have test results within minutes or even hours? There are such tests. We need millions of them.
Hydroxychloroquine: Some Answers
By Shlomo Maital
What is the truth about hydroxychloroquine, the drug that is alleged to be helpful in treating coronavirus? This piece from the New York Times may be helpful.
What is hydroxychloroquine?
Hydroxychloroquine is a prescription medicine that was approved decades ago to treat malaria. It is also used to treat autoimmune diseases like rheumatoid arthritis and lupus. It is sometimes referred to by its brand name, Plaquenil, and is closely related to chloroquine, which is also used to treat malaria.
Why has hydroxychloroquine even been considered as a possible treatment for the coronavirus?
There are several reasons. A promising laboratory study, with cultured cells, found that chloroquine could block the coronavirus from invading cells, which it must do to replicate and cause illness. However, drugs that conquer viruses in test tubes or petri dishes do not always work in the human body, and studies of hydroxychloroquine have found that it failed to prevent or treat influenza and other viral illnesses.
Reports from doctors in China and France have said that hydroxychloroquine, sometimes combined with the antibiotic azithromycin, seemed to help patients. But those studies were small and did not use proper control groups — patients carefully selected to match those in the experimental group but who are not given the drug being tested. Research involving few patients and no controls cannot determine whether a drug works. And the French study has since been discredited: The scientific group that oversees the journal where it was published said the study did not meet its standards.
A recent study from China did include a control group, and suggested that hydroxychloroquine might help patients with mild cases of Covid-19, the disease caused by the coronavirus. But that study had limitations: It was also small, with a total of only 62 patients, and they were given various other drugs as well as hydroxychloroquine. The doctors evaluating the results knew which patients were being treated, and that information could have influenced their judgment. Even if the findings hold up, they will apply only to people who are mildly ill. And the researchers themselves said more studies were needed.
Can hydroxychloroquine protect you from catching the virus?
There is no evidence that hydroxychloroquine can prevent coronavirus infection. However, researchers at the University of Minnesota are testing the drug in people who live with coronavirus patients to see whether it can protect them
Is hydroxychloroquine approved by the Food and Drug Administration?
Yes, but for malaria, lupus and rheumatoid arthritis, not for Covid-19. For decades, doctors have been legally allowed to prescribe it for any condition they think it might help, a practice called off-label use. However, because of hoarding and high demand for hydroxychloroquine, some states like New York have ordered pharmacists to fill prescriptions only for F.D.A.-approved uses of the drug or for people participating in clinical trials.
Is hydroxychloroquine being given to coronavirus patients now?
Yes. Many hospitals are giving it to patients because there is no proven treatment, and they hope it will help. Clinical trials with control groups have begun across the world. A nationwide trial began on April 2 in the United States; it is to enroll 510 patients at 44 medical centers. Researchers say those studies are essential to find out whether the drug works against the coronavirus. If it does not, time and money can be redirected to other potential treatments.
Is there any danger in taking hydroxychloroquine?
Like every drug, it can have side effects. It is not safe for people who have abnormalities in their heart rhythms, eye problems involving the retina, or liver or kidney disease. Other possible side effects include nausea, diarrhea, mood changes and skin rashes.
The leaders of three professional societies in cardiology warned on April 8 in the journal Circulation that hydroxychloroquine and azithromycin can each cause dangerous disruptions in heart rhythm, and they wrote, “There are very limited data evaluating the safety of combination therapy.”
If I can get hydroxychloroquine, should I take it to prevent coronavirus infection?
No, especially not without consulting a doctor who knows your medical history and what other medications you are taking. There is no proof that it works. And if it is being sold on the street or via the internet, it may be fake or unsafe.
An Arizona man in his 60s died last month after swallowing an aquarium cleaning product that had chloroquine on its label. He and his wife, who also became critically ill, had thought the product would protect them from the virus.
At this point, the best way to avoid infection is to practice the social-distancing and quarantine measures recommended by public health authorities. The Centers for Disease Control and Prevention also recommends that people wear cloth masks in public and wash their hands regularly.
Learn from Spain:
We WILL Err – but how?

By Shlomo Maital
Spain has suffered terribly from the new coronavirus. The numbers tell the tale:
Cases overview
Spain
| Confirmed
169,496 |
Recovered
64,727 |
Deaths
17,489 |
For a nation of 47 million, this is a terrible toll. It is explained in part by Spain’s late start in lockdown, and its Mediterranean open lifestyle, in the cafes and markets, during a warm spring.
But it seems to have peaked. The number of new cases peaked in Spain, at 8,000, daily, on April 2, and has now declined to about 4,000. So Spain is gradually beginning to emerge from lockdown, to revive the economy, in a planned careful and staged manner.
I think other countries should watch Spain carefully, talk to Spanish experts, learn about their plan, adapt the plan to their own nations’ needs and nature…and in general, we need a global brainstorming conference. An international Zoom of experts.
Take Korea. There has been a resurgence, there, a second wave, but not huge, 100 cases. OK – what happened? Is the immunity conferred by having the COVID-19 and recovering from it sufficient to give permanent immunity? Or can a huge dose of the virus come back and attack you again? Let’s find out from Korea.
How is Singapore handling the ‘track down those who spread it’? We will need to have a system for that, when we (many of us) return to work.
We should have a website clearing house for things countries have learned, but a credible one, with only vetted proven entries by real experts.
What do we know about this vicious viral enemy? Can we compile a COVID-19 handbook – here is what we know, and how we know it, and what the source of the data is.
And regarding emerging from the ‘shelter at home’ lockdown — Trump says this is the most important decision of his life. HIS decision? If I were an American, would I feel reassured in having TRUMP???? make the decision? When his ‘base’ is calling for the resignation of Fauci, a credible epidemiology expert, who urges caution?
We will make mistakes and already have. Trump’s January-February fumbling cost many lives. Maybe, it is best to err on the side of caution, as we emerge from lockdown. Let’s study Spain carefully.
Mukherjee: Worth Reading and Heeding
By Shlomo Maital

Siddhartha Mukherjee, MD
Who is Dr. Siddhartha Mukherjee? He is a 49-year-old Indian-American, physician, biologist, oncologist, author, TV commentator. His book on cancer won the Pulitzer Prize in 2011. He is an Associate Professor of Medicine in the Division of Hematology and Oncology, Columbia University Medical Center.
The Government of India conferred on him its fourth highest civilian award, the Padma Shri, in 2014.
His article in The New Yorker, March 26, on the pandemic is brilliant and clear. Here is a brief summary of his main points. (800 words…).
* Ancient Chinese and Indians, and Arab doctors, knew long ago, that you could ‘vaccinate’: e.g. “taking matter from a smallpox patient’s pustule and applying it to the pricked skin of an uninfected person, then covering the spot with a linen rag.” Healers in China did this as early as 1100 AD.
* Three question deserve attention: 1) “do people exposed to higher ‘doses’ of virus have increased risk of infection? (e.g. healthcare workers). 2) Is there a relationship between the ‘dose’ of virus and the severity of the disease?” 3) “can exact quantitative measures of how the virus behaves in infected patients (peak viral load, patterns of its rise and fall…) predict the severity of the illness, and its infectiousness to others? We need to start measuring the virus WITHIN people!”
The fact that we do not have strong proven answers to these questions, show how little we really know about COVID-19 and how we are fighting in the pitch dark!
For HIV, Mukerjee notes, how much was in a patient’s blood produced a distinct pattern; the virus count in the blood rises to a peak “Peak viremia”, patients with the highest peak viremia “typically became sick sooner, they were least able to resist the virus.” (Same goes for coronavirus? We don’t know). The set point too is crucial (the level to which a virus count settles and stabilizes, after its initial peak. People with a high set point move quicker to actuall AIDS (autoimmune disease). Same for COVID-19? Also, viral load (quantity of the virus in the body) helped predicts (AIDS’) nature, course and transmissibility. (Same for COVID-19?)….
For kids – could an initial low-level exposure (as the ancient Chinese Indians and Arabs did) lead to a lower set point, (and hence less COVID-19 danger and risk?)….
Mukherjee cites research showing “the more virus you shed, the more likely you are to infect others” from HIV research. I.e., the R0 number (numbers infected by one infected person) is variable, depending on how much virus the infected person ‘sheds’.
“Does a large viral dose result in more severe disease? “For reasons we don’t understand front-line healthcare workers are at greatr risk for serious illness despite their younger age.” Is it because they are exposed to ‘higher doses’? (Correlation between dose and severity varies widely from one strain of flu to the next). Corona viruses “seem to follow the pattern seen in influenza”. A SARS study showed (in Hong Kong) that “a higher initial load of virus measured in the deep part of your throat above your palate was correlated with more severe respiratory illness”. For measles, there is proven links between dose and severity.
Finally, can we track viral load and hence predict the course of the disease? Here’s the catch. Tests are done with oral swabs. But viral dose varies immensely with how the oral swab is administered, and it varies tremendously among doctors and healthcare workers who administer the swab! A study in the Lancet medical journal does show that “viral loads…from patients with severe COVID-19 were 60 times higher on average than loads among patients with a mild form of the disease”!.
Data. Bring me data. We need to know how much virus COVID-19 patients harbor, not just whether they harbor any.
“If we had “dosimetry” (viral dose measures), we can quarantine those who are most infectious.”
Let’s do a two-step procedure. 1. Identify infected patients. 2. Quantify viral loads in nasal or respiratory secretions. Plan medical care accordingly.
End Lockdown? Mukherjee says, we need two criteria: people have no measured viral shedding, and they have signs of persistent immunity in their blood (antibody test). Healthy immune workers are crucial – they can work with no danger to themselves or others, and they can care of other sick people!
Why should we listen to an oncologist? “Measurement and enumeration are the mainstays of medicine for people in my field. We do ‘risk stratification’. “ This should be the case for treating COVID-19 too.
Mukherjee makes a simple medical point. “To win the (battle) against COVID19, it is essential to trace the coure of the virus as it moves through the populations. But it’s equally essential to measure its course within a single patient. The one becomes the many. Count both; both count.”
Emerging from Virus:
Academics Step Up
By Shlomo Maital
Public health officials, who are in control in most countries, have their hands full, dealing with the medical crisis. So it is up to us, academics and others, to begin weighing options for emerging from the lockdown.
An interuniversity team led by Tel Aviv U. President Ariel Porat and Weizmann Institute President Alon Chen, have prepared an excellent 27-page plan. Details are reported by Haaretz journalist Meirav Arlosoroff.
(Suggestion to other countries: why not set up a similar team? Include epidemiologists, virologists, economics, psychology, law, computer science, even quantitative physics, and of course public health).
Here are the options the experts present. Option One: Maintain the strick lockdown. Option Two: the opposite, speed up the rate of infection among Israel’s non-vulnerable population (is there such a thing?) to achieve ‘herd immunity’ (VERY bad term – we are NOT a herd… why not population immunity? Or mass immunity?). Under the second option, the elderly would remain in isolation for their protection.
Neither are very attractive, are they? There is a missing link – widespread testing, to provide detailed data. The required number of tests is not available.
So the committee suggests a third option — a “gradual lifting of the lockdown while officials carefully monitor numbers related to the pandemic. Divide Israel into equally sized ‘risk zones’ based on how far and wide the coronavirus has spread. Red zones would maintain total lockdown. Yellow zones would be where people are allowed to leave their homes for work, provide they stay inside the yellow zone! In Green Zones residents are free to go to their jobs, including jobs outside their zone. Those showing symptoms remain in quarantine in all three zones. Those shown to be immune are free to go wherever they please. (A key here is a serological antibody test, not yet widely available) Places of work would reopen, subject to strict rules on hygiene and social distancing. Workplaces would be graded, according to how risky they are for a ‘second wave’ outbreak. Workplaces barred from opening would be exempt from rent.
The committee also recommended tax incentives to encourage work from home.
Division into red, orange, green zones is based on sophisticated mathematical models that predict the epidemic’s spread – along with high levels of testing. Sampling tests that show less the 2-3% infection rates would enable ease of the lockdown. Green zones are where the number of serious cases doesn’t exceed 100 and the infection rate is less than 8 %. Technologies like location technology and artificial intelligence will be used to predict the possible rate of contagion.
Since test kits are in short supply, a model for sampling should be used, for each cone, including children, so schools can reopen.
The Committee says that a measured exit from the lockdown can and should already begin. It calls for allowing between 900,000 and 1.5 million workers to return to their jobs. This is between one quarter and a third of Israel’s work force.
“Data from the math models shows that the virus’ high infection rate does not allow for complete release from lockdown, even for Green zones”, they note. Social distancing still is the main tool, to reduce infection parameters by a factor of 2 to 3. Areas of especially high infection must receive special treatment, such as the ultra-Orthodox areas.
I believe that each country needs its own inter-University committee of this sort, because each country has its own culture and unique circumstances. It needs to be a non-governmental civilian effort, because governments are simply focused on the day-to-day.

