
You are currently browsing the tag archive for the ‘COVID-19’ tag.
COVID-19 & Culture
By Shlomo Maital

All over the world, nations are undergoing lockdown – or versions of it, “shelter at home’ (a term used in the US for what you do when a possible tornado or hurricane threatens), quarantine (a French word for ‘40’, based on the 40 days people were closed off during plague), or even curfew.
It does seem that nations where quarantine was earliest, and most heeded, did the best. Places or countries that heeded quarantine the least and latest did worst.
In Israel, COVID-19 afflicts heavily the ultra-Orthodox, partly because in early March Purim celebrations brought masses of them together and spread the plague.
In Wuhan a 70-day lockdown, rigidly enforced, seems to have done the trick.
In Michele Gelfand’s new book (she is a professor at U. of Maryland), the difference between countries with rule breakers and rule makers is explored. This is highly relevant for our coronavirus dilemma.
Brazilians are rule breakers. Society is “loose” and relaxed. So is Israel. Try driving on our roads and highways. Rules here are made to be broken. This is somewhat strange, because countries that have lived under threat, invasion and natural disasters tend to be rule making and rule observing (Japan!). Not Israel.
Singapore is a rule maker. Don’t bring 200 packages of gum into the country. Don’t toss your old gum onto the street. You get fined. Singapore has handled the plague very well. So has South Korea, a rule maker society. Brazil’s new President seems to ignore it.
In Israel, the virus is reaching its apex, roughly around today. A severe police-enforced lockdown was declared just before Passover, because families in Israel always get together to observe and celebrate it. So police set up roadblocks and levied heavy fines, for those trying to travel. In rule breaking nations, to enforce a rule you really do need the police and fines, and even the Army (used in ultra-orthodox areas in Israel).
Is your country a rule maker or a rule breaker? And how is it dealing with the lockdown? Will it change the culture of your country? Will it become more submissive – or return to its old loose ways soon after?
New York City residents are definitely rule breakers. But strenuous efforts have kept them mainly locked down. In the southern parts of the US, political leaders seem to have barely even tried.
- – – – – – –
“Rule Makers, Rule Breakers provides an extremely insightful and increasingly important understanding of human cultures. It distills years of scientific research on the cultural differences in the strength of social norms, or tightness-looseness, in a cohesive and engaging way and shows how it informs politics, class differences, workplaces, and other facets of our world. Even more importantly, it shows how this cultural difference springs from the presence (or absence) of environmental instability and threat. If you’ve ever wondered why some cultural groups are so lax while others are so stringent or why working-class parents often tend to be stricter than middle-class parents, this book holds the answers. Ultimately, the best part of this book is that it provides a cohesive and informative framework for interpreting world events and human behavior that will prove useful for years to come. If you enjoyed Guns, Germs, and Steel or have an appreciation for the topics of social science, history, psychology, or culture, you’ll love this book”.
from an Amazon review
Mukherjee: Worth Reading and Heeding
By Shlomo Maital

Siddhartha Mukherjee, MD
Who is Dr. Siddhartha Mukherjee? He is a 49-year-old Indian-American, physician, biologist, oncologist, author, TV commentator. His book on cancer won the Pulitzer Prize in 2011. He is an Associate Professor of Medicine in the Division of Hematology and Oncology, Columbia University Medical Center.
The Government of India conferred on him its fourth highest civilian award, the Padma Shri, in 2014.
His article in The New Yorker, March 26, on the pandemic is brilliant and clear. Here is a brief summary of his main points. (800 words…).
* Ancient Chinese and Indians, and Arab doctors, knew long ago, that you could ‘vaccinate’: e.g. “taking matter from a smallpox patient’s pustule and applying it to the pricked skin of an uninfected person, then covering the spot with a linen rag.” Healers in China did this as early as 1100 AD.
* Three question deserve attention: 1) “do people exposed to higher ‘doses’ of virus have increased risk of infection? (e.g. healthcare workers). 2) Is there a relationship between the ‘dose’ of virus and the severity of the disease?” 3) “can exact quantitative measures of how the virus behaves in infected patients (peak viral load, patterns of its rise and fall…) predict the severity of the illness, and its infectiousness to others? We need to start measuring the virus WITHIN people!”
The fact that we do not have strong proven answers to these questions, show how little we really know about COVID-19 and how we are fighting in the pitch dark!
For HIV, Mukerjee notes, how much was in a patient’s blood produced a distinct pattern; the virus count in the blood rises to a peak “Peak viremia”, patients with the highest peak viremia “typically became sick sooner, they were least able to resist the virus.” (Same goes for coronavirus? We don’t know). The set point too is crucial (the level to which a virus count settles and stabilizes, after its initial peak. People with a high set point move quicker to actuall AIDS (autoimmune disease). Same for COVID-19? Also, viral load (quantity of the virus in the body) helped predicts (AIDS’) nature, course and transmissibility. (Same for COVID-19?)….
For kids – could an initial low-level exposure (as the ancient Chinese Indians and Arabs did) lead to a lower set point, (and hence less COVID-19 danger and risk?)….
Mukherjee cites research showing “the more virus you shed, the more likely you are to infect others” from HIV research. I.e., the R0 number (numbers infected by one infected person) is variable, depending on how much virus the infected person ‘sheds’.
“Does a large viral dose result in more severe disease? “For reasons we don’t understand front-line healthcare workers are at greatr risk for serious illness despite their younger age.” Is it because they are exposed to ‘higher doses’? (Correlation between dose and severity varies widely from one strain of flu to the next). Corona viruses “seem to follow the pattern seen in influenza”. A SARS study showed (in Hong Kong) that “a higher initial load of virus measured in the deep part of your throat above your palate was correlated with more severe respiratory illness”. For measles, there is proven links between dose and severity.
Finally, can we track viral load and hence predict the course of the disease? Here’s the catch. Tests are done with oral swabs. But viral dose varies immensely with how the oral swab is administered, and it varies tremendously among doctors and healthcare workers who administer the swab! A study in the Lancet medical journal does show that “viral loads…from patients with severe COVID-19 were 60 times higher on average than loads among patients with a mild form of the disease”!.
Data. Bring me data. We need to know how much virus COVID-19 patients harbor, not just whether they harbor any.
“If we had “dosimetry” (viral dose measures), we can quarantine those who are most infectious.”
Let’s do a two-step procedure. 1. Identify infected patients. 2. Quantify viral loads in nasal or respiratory secretions. Plan medical care accordingly.
End Lockdown? Mukherjee says, we need two criteria: people have no measured viral shedding, and they have signs of persistent immunity in their blood (antibody test). Healthy immune workers are crucial – they can work with no danger to themselves or others, and they can care of other sick people!
Why should we listen to an oncologist? “Measurement and enumeration are the mainstays of medicine for people in my field. We do ‘risk stratification’. “ This should be the case for treating COVID-19 too.
Mukherjee makes a simple medical point. “To win the (battle) against COVID19, it is essential to trace the coure of the virus as it moves through the populations. But it’s equally essential to measure its course within a single patient. The one becomes the many. Count both; both count.”
The Coronavirus Vaccine Will Be French:
Meet Prof. Frederick Tanji
By Shlomo Maital

Prof. Frederick Tanji
“Louis Pasteur wa born on December 27, 1822 –and died on September 28, 1895. He was a French biologist, microbiologist and chemist renowned for his discoveries of the principles of vaccination, microbial fermentation and pasteurization. He made remarkable breakthroughs in the causes and prevention of diseases, and his discoveries have saved many lives ever since. He reduced mortality from puerperal fever and created the first vaccines for rabies and anthrax.” The Pasteur Institute in Paris, named after him, is a world leader in this field.
Fast forward. Prof. Frederick Tanji is a senior professor at the Pasteur Institute in France and the head of the Department of Virology at the National Institute of Scientific Research (CNRS). He works day and night on developing a vaccine against a corona virus, and is one of the top candidates to get to the finish line first.
According to press accounts, “Tanji’s development team received € 4.3 million in funding to start clinical trials for the corona vaccine he developed, which, like others developed at the institute, is based on measles vaccine. “I developed a measles vaccine given to every baby born, which is effective and safe,” Tanji explains. “All the vaccine makers in the world know how to produce this vaccine in large quantities – which is very important. It’s also very cheap. This vaccine can be used as a (vector) basis for the Corona vaccine. I have engineered the measles virus genome so pathogenic sequences can be added to it. Like other viruses. That’s what we’re doing now with the Corona virus. “
“Tanji’s method – based on measles vaccine – has already been applied to other vaccines that have undergone clinical trials and some are already in production, and are designed to prevent Zika’s disease, Lassa fever, 1SARS, and MERS, “so we already have experience developing corona vaccine vaccines “, Says Tanji.
If Tanji succeeds, we need to thank the Chinese. “The speed at which vaccine development researchers came to be due in part to the early and rapid Chinese effort to sequence the genome of the new virus. China shared the genetic information in early January, allowing distance groups around the world to grow and investigate a live virus.”
Tanji wants the vaccine to be produced and sold at cost.
Tanji thinks human behavior will have to change radically post-COVID-19. “Social behavior will have to change, and we will have to significantly reduce travel. 4 billion people are flying every month – half the world’s population, that’s crazy. It transmits diseases. The economy needs to change.”
Beware of the Second Wave!
By Shlomo Maital

As the ‘rate of doubling’ (number of days COVID-19 cases double, from every three days to weekly or more) slows, in some countries, even plague-ridden ones like Italy, a new danger emerges: Complacency.
Writing in the New York Times, Nicholas Kristof warns of a second wave.
“….countless thousands will still die because of past mistakes and complacency. A pandemic is like an oil tanker: It continues to move forward long after you hit the brakes. In China, deaths didn’t fall sharply until a month after controls had been imposed. The benefits from social distancing in the United States will take time to ripple through the system, and there will continue to be new infections — and many more deaths.
Kristof continues: “The Institute for Health Metrics and Evaluation at the University of Washington has a constantly updated model that predicts that the daily death toll across the United States will rise until April 16 and then slowly decline. By the beginning of August, it estimates that more than 93,000 Americans will have died from Covid-19.”
“More bad news: Case fatality rates have been creeping up, and lethality may be greater than many had expected. Germany was hailed for a death rate of only about 0.5 percent, and South Korea was not much higher; now both have case fatality rates well above 1 percent. In models of the virus that my colleague Stuart A. Thompson and I published, we used a death rate of 1 percent. But if the South Korean death rate by age is applied to the demography of the United States, the American case fatality rate is about 2 percent, according to Dr. Christopher Murray, the director of the Institute for Health Metrics and Evaluation.
“A great majority of the deaths in the United States will have been avoidable. South Korea and the United States had their first coronavirus cases on the same day, but Seoul did a far better job managing the response. The upshot: It has suffered only 174 coronavirus deaths, equivalent to 1,100 for a population the size of America’s.
“That suggests that we may lose 90,000 Americans in this wave of infections because the United States did not manage the crisis as well as South Korea did. As of Friday night, the U.S. had already had more than 7,000 deaths. ….. while we can bend the curve, it will bend back when we relax our social distancing.
“This is more bad news, for many people seem to believe that once we get through this grim month or two, the nightmare will be over. But the virus is resilient, and health experts warn that this may be just the first wave of what may be many waves of infections until we get a vaccine sometime in 2021.
“We’re just looking at this first wave,” noted Dr. Murray. He estimates that in June, some 95 percent of Americans will still be susceptible to the virus. “The world’s on fire with this virus,” said Michael Osterholm, an epidemiologist at the University of Minnesota, and this means that even if one country succeeds in putting out the blaze, sparks will keep arriving from elsewhere to cause new outbreaks. He added: “I think the transmission will continue to occur for some time.”
COVID-19: The Rule of 72 Rules
By Shlomo Maital
Albert Einstein once said famously, that compound interest is the “most powerful force in the universe.” It is indeed, especially when compound interest is at work, in transmitting virus from one person to another, at varying rates.
So, here is the Rule of 72, and some optimistic news from my country Israel.
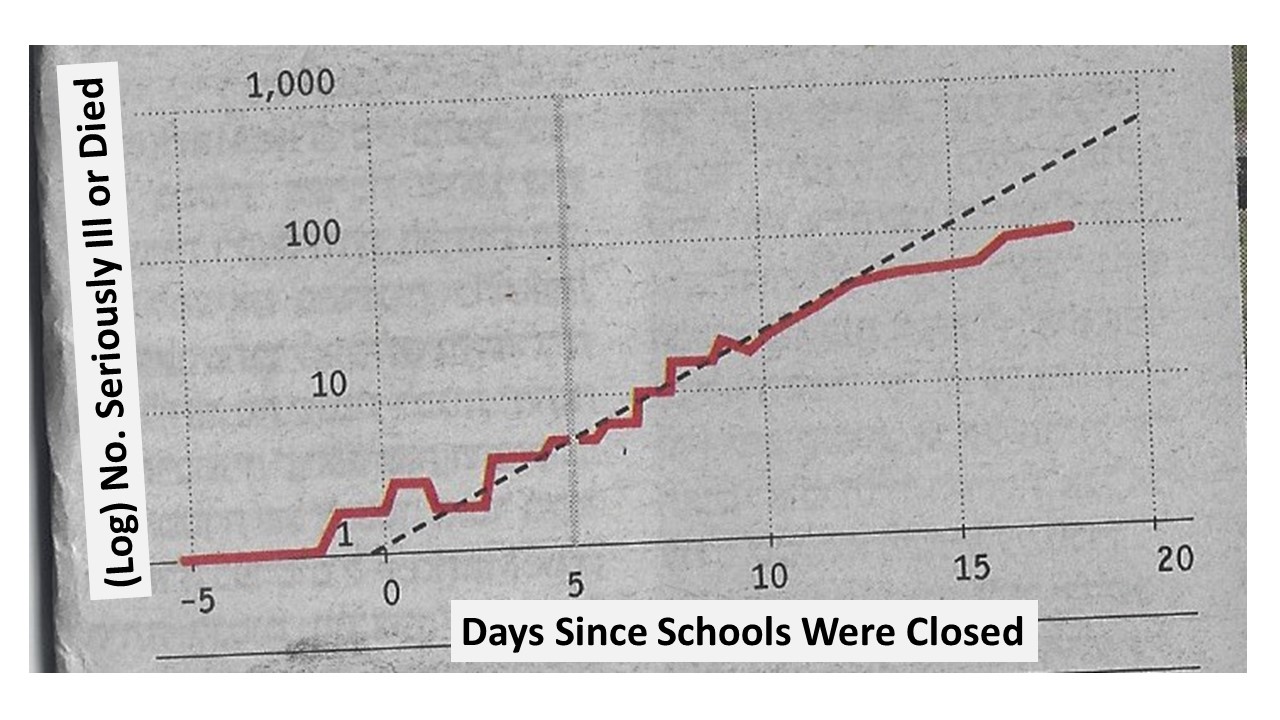
How fast is the number of infected persons doubling? How often? Are we succeeding in slowing it? The graph above shows the number seriously ill, or who have died, from COVID-19, in Israel, dated from when schools closed – and the dotted line shows the future projection. The data are by the National Security Council.
Initially, it was assumed that the daily growth in COVID-19 seriously ill and deaths was growing at a compounded interest rate of 25% daily !! (why compound: because 25% more people, infect 25% more people, infect 25% more people..and so on…like bank compound interest).
Here is the Rule of 72: The Rule of 72 shows you how quickly you’ll double your money. All you have to do is divide 72 by the interest rate it’s earning. This is the number of years it will take for your money to double.
Translate that to virus: Divide 72 by the daily rate of increase at which people fall seriously ill or die – that tells how rapidly the number of victims doubles – in how many days. 25% daily growth? 72/25 = about 3. Every 3 days. So in one month, 30 days, we have 10 doublings. 2 raised to the 10th power is 1,024. A thousand times more ill and dead, in one month. Simply not a situation hospitals can handle.
And that was the initial doubling rate in Israel, in the early days of school closure. Then people got the message and sheltered at home.
The daily infection rate then declined, to 15%. According to the National Security experts.
What does that mean? Rule of 72: 72/15 or about 5. Doubling every five days. How many doublings in 30 days? 30/5 equals 6. Two to the 6th power equals 64.
Sixty-four times more victims.
Something we can handle. Difficult, tragic – but – do-able.
Sixty-four times more victims is hugely better than 1,024 times more victims.
This is the Rule of 72. And the key point is – the Rule of 72 is in OUR hands. As my cell phone tells me each time I open it: Stay Home. Getting the ‘compound interest’ rate down from 25% to 15% is hugely valuable. When we invest we want more interest; when we shelter, we want a whole lot less (virus spread). And even small differences in the rate of spread make a huge improvement.
Now – next step, how do we figure out who can emerge from home to run the factories and farms? And when? But so far, the Rule of 72 Rules.
A Vaccine Is On The Way – Soon?
By Shlomo Maital

Today’s Jerusalem Post daily paper, published in Jerusalem, brings some much-needed good news about progress in creating a vaccine against COVID-19.
The report notes:
“A team of Israeli researchers says that they are days away from completing the production of the active component of a coronavirus vaccine that could be tested on humans as early as June 1. “We are in the final stages and within a few days we will hold the proteins – the active component of the vaccine,” Dr. Chen Katz, group leader of MIGAL’s biotechnology group, told The Jerusalem Post. In late February, MIGAL [The Galilee Research Institute] committed to completing production of its vaccine within three weeks and having it on the market in 90 days. Katz said they were slightly delayed because it took longer than expected to receive the genetic construct that they ordered from China due to the airways being closed and it having to be rerouted.”
(Note: the ‘genetic construct’ from China, is simply the RNA ribonucleic acid that defines COVID-19 — shame that cancellation of flights from China to Israel caused the delay – every day counts!).
“As a reminder, for the past four years, researchers at MIGAL scientists have been developing a vaccine against infectious bronchitis virus (IBV), which causes a bronchial disease affecting poultry. The effectiveness of the vaccine has been proven in preclinical trials carried out at the Veterinary Institute.”
Amazing that chickens, maybe, and their vaccine can help save human lives?
The report continues: “Our basic concept was to develop the technology and not specifically a vaccine for this kind or that kind of virus,” said Katz. “The scientific framework for the vaccine is based on a new protein expression vector, which forms and secretes a chimeric soluble protein that delivers the viral antigen into mucosal tissues by self-activated endocytosis, causing the body to form antibodies against the virus.”
What does this mean? Basically: The vaccine helps the body produce a key protein able to penetrate the cells infected by COVID-19 in the throat and lung mucous. How does it penetrate? Endocytosis is “the process of actively transporting molecules into the cell by engulfing it with its membrane.” This helps the cell produce antibodies that kill the virus, before it can kill the cell and reproduce, creating millions of new viruses that spread through the lungs.
“In preclinical trials, the team demonstrated that the oral vaccination induces high levels of specific anti-IBV antibodies, “ a MAGAL expert said.
A worldwide race is on, to develop an effective safe COVID-19 vaccine. Whoever wins, humanity will be the big winner. This is one race that can benefit everyone, even the spectators.
Save the Theodore Roosevelt!
By Shlomo Maital

USS Theodore Roosevelt Aircraft Carrier
Many years ago, my son Ronen, then an officer and chief engineer on an Israeli missile boat, and I boarded an American Sea Stallion helicopter at Ben Gurion Airport, Tel Aviv, and were ferried to the enormous American nuclear aircraft carrier Theodore Roosevelt, anchored a few miles offshore. (The ship was far too big to enter Haifa Port).
This was made possible by my cousin Malcolm, then a nuclear sub commander. Thanks again, Mal!
Ronen and I were astounded. Eleven decks, 5,000 sailors, nuclear engines meant it could stay on duty for many months, 80 jet aircraft launched from the upper deck, and the ability to launch and receive planes at the same time – and the capability, practiced frequently, of launching and recovering in the dark of night (not done by other nations).
Wow.
Fast forward. COVID-19. A New York Times article reports: Captain of Aircraft Carrier Pleads for Help as Virus Cases Increase Onboard. “We are not at war,” the captain of the carrier Theodore Roosevelt wrote. “Sailors do not need to die. If we do not act now, we are failing to properly take care of our most trusted asset — our sailors.”
The ship was then in Guam. Hospital facilities there are very very limited.
In a four-page letter dated Monday, first reported by The San Francisco Chronicle on Tuesday, Capt. Crozier laid out the dire situation unfolding aboard the warship, the Theodore Roosevelt, which has more than 4,000 crew members. He described what he said were the Navy’s failures to provide him with the proper resources to combat the virus by moving sailors off the vessel. “We are not at war,” Captain Crozier wrote. “Sailors do not need to die. If we do not act now, we are failing to properly take care of our most trusted asset — our sailors.”
(The Acting Secretary of the Navy has responded that, well, nobody on the ship is really THAT ill… so — suck it up, guys!)
“Thomas B. Modly, the acting Navy secretary, told CNN in an interview that the Navy was working to move sailors off the ship — but that there were not enough beds in Guam to accommodate the entire crew.”
“We’re having to talk to the government there to see if we can get some hotel space, create some tent-type facilities there,” Mr. Modly said. “We’re doing it in a very methodical way because it’s not the same as a cruise ship.”
Speaking to reporters Tuesday night, the commander of the Pacific Fleet, Adm. John C. Aquilino, said that “we’re welcoming feedback” regarding the requests outlined by Captain Crozier. Admiral Aquilino said that crew members would be rotated off the carrier for testing and quarantine before returning aboard. The intent, he said, was to keep the ship ready to carry out its missions. He said that no crew members had been hospitalized thus far, but he declined to specify the number of infections.
“The problem aboard the Roosevelt highlights a central dilemma facing the military: Top officials, who have spent years placing readiness to fight the next war as a top priority, are now finding that maintaining that readiness during a pandemic can endanger the health, and even the lives, of service members. At the same time that Americans are being told to stay at home and practice “social distancing” in public, many service members are instead being told to continue doing their jobs.”
I find this episode infuriating! I’ve served in military reserves and trained hard. Be ready to fight, is the credo. True. But in times of pandemic plague? Save lives. And soldiers’ lives matter too.
Anyone want to start a Twitter account, Soldiers’ and Sailors’ Lives Matter? Because they do.
Wake up, Defense Secretary Mark Ester. You can save the lives of the sailors on the Theodore Roosevelt. These young men and women, some only 19 years old, spend long months at sea, away from their families. In normal times they defend America, all over the world. But now? It is urgent, top priority, to save their lives.
So – do something! DO SOMETHING! If you do not, their lives are your responsibility. And there will be no forgiveness.
COVID-19: Logarithms Hold the Key
By Shlomo Maital

Warning: This blog could be harmful to your health…because it’s about… logarithms. (Logs). And plague. What in the world?
Well, let’s give it a shot. Nothing to lose.
A logarithm is a number, such that when its ‘base’ (usually, the number ten, or the number ‘e’, 2.71828 (we do NOT have to go into the black depths of THAT number), is raised to the value of the log, you get the value of your starting number, x.
For instance, 102 = 100. So the logarithm of 100 (using the ‘base’ of 10) is 2.
Clear?
Why are logarithms useful? Well, they have fallen into massive disuse lately, because of computers and calculators. But once they were crucial. Because, suppose you need to multiply two big numbers. On paper. Ouch! But wait! If you knew the logarithms of the two numbers? Add them! Because? The value of by times bz equals bz+y — so, we have converted multiplying (hard!) to addition (easy!).
Logarithms was publicly proposed by John Napier in 1614, an English mathematician. Generations of school children (like my mother) had to learn the secrets of logs.
But what has this to do with COVID-19. So – there is a wonderful magical property of logs. Suppose there is a key number that you are tracking. E.g., the number of people in your country or your city or community, who have COVID-19. You can graph it, look at it, inspect the curve, it is rising, OK, but – what does it mean?
So here is what John Napier would recommend, 400 years ago. Take the logarithm of the number. Graph THAT, not the number itself.
Why? Because – trust me on this — the gradient, (steepness, or slope) of the logarithm graph tells everything. If the slope of the log is RISING, then the RATE of increase is increasing. If the slope is getting less steep, FALLING, the rate of increase of COVID-19 is declining. And this is crucial, to know how we’re doing. And you CANNOT tell this is you graph the number itself.
So, here in Israel, the slope of the logarithm of the number infected with COVID-19 has been declining. Yay! The rate of increase is declining. We’re getting toward the apex. It’s a ways off…but once we reach the top of THAT hill, the slope of the log will turn from positive to negative…and that’s a KEY point. Because that’s when the number infected begins to fall….cause of celebration.
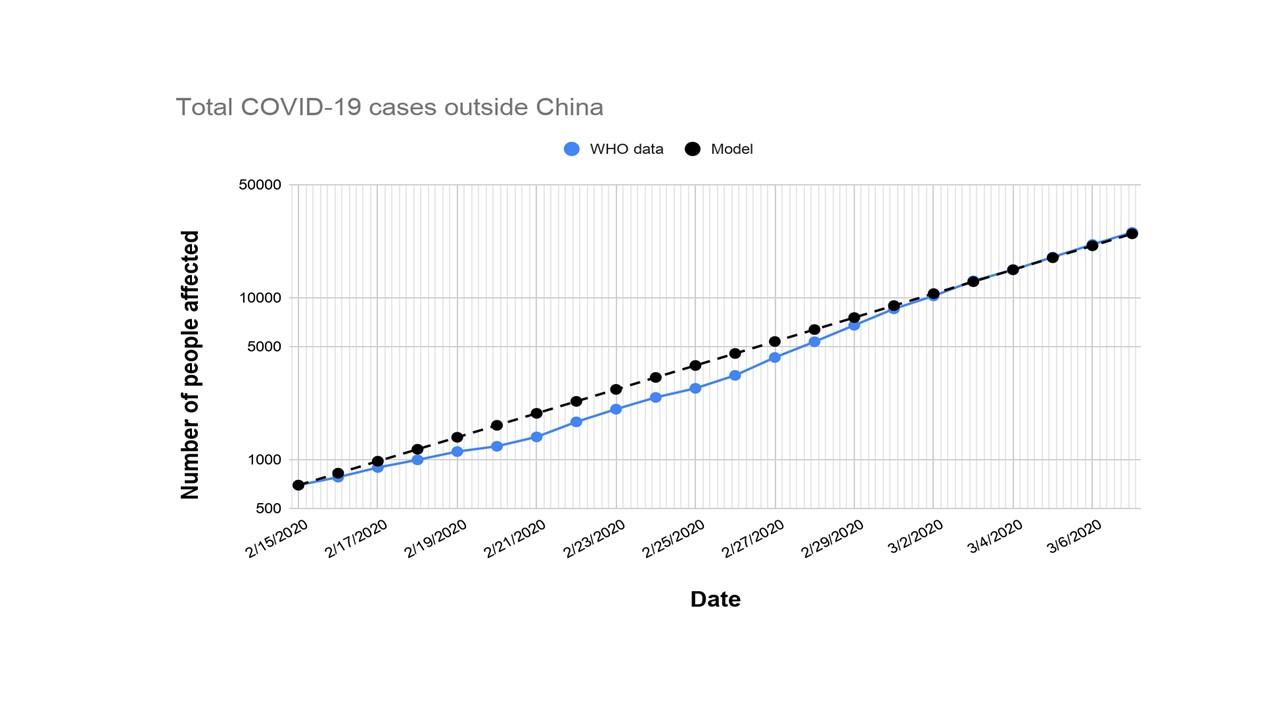
Clear? Clear as mud? So here is a sample graph. This is the total number of cases outside China. On a log scale. You can see a constant slope – constant rate of growth, as the virus spreads. Reflecting, maybe, a very slow response in Europe and the US.
So – in your country or city, track the logarithm of the number of cases, and measure the slope. That tells you whether it is speeding up or slowing down. I don’t think our political leaders are quite up to that difficult mental exercise.
How the US Screwed Up:
A Litany of Fumbles
By Shlomo Maital

Ooops…fumbled the ball!
The United States, led by the Trump administration, has fumbled the ball in dealing efficaciously with the COVID-19 pandemic. Here is the terrible litany of fumbles, mistakes and bad decisions, which in the end cause the deaths of many people. Needlessly.
April 2018. Some nine or ten months before the crisis arose, Trump and his National Security Council advisor John Bolton (later fired himself…justice?) fire the NSC team charged with pandemic preparation; on April 8 Tim Bossert is fired, as Home Secretary Advisor, in charge of “comoprehensive defensive strategy against pandemics”. Bye bye strategy and plans. In May Rear Amiral Tim Ziemer, who headed a ‘health security team’ was fired and not replaced.
Fast forward: China experiences early COVID-19, and, rather late, in late December, informs the world of it, and warns. On Jan. 20 the Center for Disease Control, in the US, announces the first case, a traveler from Wuhan, China. “We shut it down”, Trump says on Feb. 2. In February the CDC sends out its COVID-19 test, to public health testing labs in the US states; it doesn’t work. The US, (pride? Ego?) fails to purchase tests that are proven to work, from South Korea and other countries. The test is fixed, finally – but valuable weeks are lost. The public health labs work at developing their own test, something that has never before happened.
“When the CDC rolled out its tests, a component in them turned out to be faulty. That was unfortunate, but it put a big spotlight on the CDC’s decision to use its own test kit instead of test kits other countries have used, reportedly in an effort to create a more accurate test.”
As of March 9, well into the US pandemic, only 4,300 COVID-19 tests had been carried out. Trump says, “the tests are perfect” (like his phone call to the Ukrainian President).
Press reports: “Testing is crucial to slowing epidemics. First, it lets public health officials identify sick people and subsequently isolate them. Second, they can trace that sick person’s recent contacts to make sure those people aren’t sick and to get them into quarantine as well. It’s one of the best tools we have for an outbreak like this. It’s also something that the federal government has done well before — recently, with H1N1 and Zika. “It’s been surprising to me that the administration’s had a hard time executing on some of these things,” Ashish Jha, director of the Harvard Global Health Institute, said. “
America dropped the ball on testing. Press reports: “In the months before the coronavirus outbreak, the administration cut a public health position that was meant to help detect disease outbreaks in China, where the pandemic began, Even without such cuts, experts and advocates argue the US generally underfunds disease outbreak preparedness and public health programs more broadly. Further cuts just deepen the risks of pandemics. The common refrain among experts is that other countries’ actions, such as China’s draconian measures, gave the US a bit of time to do something, but the federal government has failed to get even the basics right in that time.”
What was President Trump’s role in this? “Trump “did not push to do aggressive additional testing in recent weeks, and that’s partly because more testing might have led to more cases being discovered of coronavirus outbreak, and the president had made clear — the lower the numbers on coronavirus, the better for the president, the better for his potential re-election this fall.”
Hospitals, especially in New York City, complain they lack equipment. Why? There is a large US strategic stockpile of lots of useful things. However, “While the administration has said it’s using federal authorities and tapping into its stockpiles to get more of this gear to the places that need it, health care workers on the ground complain that they still don’t have enough — forcing them to reuse possibly contaminated equipment and choose between working in unsafe conditions or not show up to work at all. All of this at a time when the country needs to, according to experts, boost health care capacity.” There are rumors, Trump dislikes Washington state and New York State and that this is impacting federal shipments.
In a pandemic, preparedness is crucial. The US Defense Department has contingency plans for a huge variety of threats. What about the health area? “….. this reflects on the lack of preparedness: A shortage of medical equipment is one of the many problems government simulations and exercises warned about before the current outbreak. But Trump simply didn’t prioritize pandemic preparedness beforehand. The US … was not prepared … A good preparedness plan would have helped address this and had things in place to allow for that increased need to be met.”
US health care system is inadequate, even with Obamacare (imagine if Trump had succeeded in annulling it!?). “With the outbreak growing, the US’s lack of universal health care has become an even more obvious problem: If people can’t get testing, they’re less likely to find out they have Covid-19 and take precautions to avoid spreading the virus. If they can’t get treatment in case of complications, they’re more likely to suffer, potentially spread the disease, and die.”
Fighting the poor, rather than the virus: “The administration has pushed forward on measures that will kick people off food stamps. This will not only lead people to suffer if they lose their jobs as a result of a coronavirus-caused recession, but it could lead to sick people going to work and spreading the disease, because they won’t have a safety net if they don’t bring in a paycheck.”
Chasing immigrants, instead of virus: “Experts also pointed to the “public charge” rule, which effectively discourages immigrants from seeking public services, including health care, by threatening their immigration status if they are “likely to be a public charge” by relying on those services.”
Yes, the United States has dropped the ball – fumbled it. And this litany is very very partial – it’s only 1,000 words, it could fill a book.
And the sad part, again, is that when a halfback fumbles in football, worst case, his team loses the game. In the US, when the administration fumbles, people die. Many people. And then ? Excuses. Boy, are we going to hear excuses, all the way to November and beyond.
Dr. Anthony Fauci predicts, as many as 200,000 Americans could die in this pandemic. Many of these deaths could have been prevented, if the Administration had simply held onto the ball.
There has to be accountability. At the very least, at the ballot box in November.
Meet Andrea Ray: Heroine
By Shlomo Maital

In our pandemic crisis, there are a huge number of unsung everyday heroes. Truck drivers who continue to drive the long hauls, delivery people, supermarket workers, police, Israel’s Home Front soldiers….
And, in particular, Andrea Ray, featured on Channel 12 this evening. Andrea was born in Venezuela and made Aliyah to Israel when she was 16. She studied hotel management and had a senior job in the Dan Hotels system.
Israel has taken over some of the Dan Hotels in Tel Aviv, and brought those who have tested positive for COVID-19, especially those flown home from abroad, to hotels. The area housing these patients is of course strictly quarantined, and the hotel is run jointly by the Home Front soldiers and Dan management.
Why is Andrea a hero? Who will care for the corona patients? Seriously? Spend many hours of the day mingling with those ill with the deadly virus?
You cannot tell someone to do this. You can only ask for volunteers.
And Andrea volunteered. This is what she does, every day, for hours and hours – cares for the needs of the patients, cheers them up, laughs with them, and brings them joy with her smile.
What if she falls ill? Well, I’ll get the virus and then I’ll get better, she says.
So, you’ve met Andrea Ray, heroine. Do you know other such heroes and heroines?

